Download as PDF, PPTX
![EMPHYSEMA
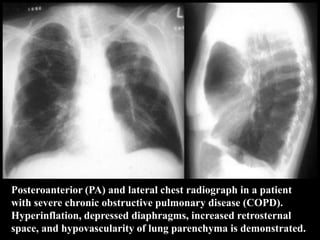
[COPD - CHRONIC OBSTRUCTIVE
PULMONARY DISEASES]
Dr.CSBR.Prasad, M.D.](https://image.slidesharecdn.com/emphysema-csbrp-130111113343-phpapp02/85/Emphysema-1-320.jpg)

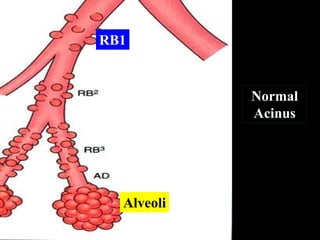
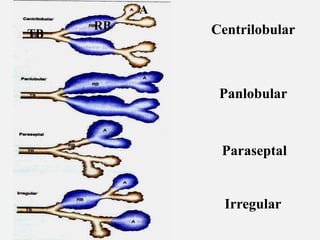
![Classification: Types of emphysema
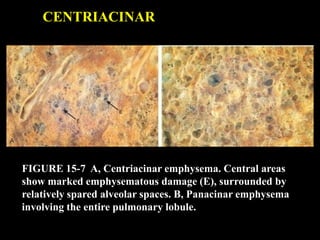
1. Centriacinar
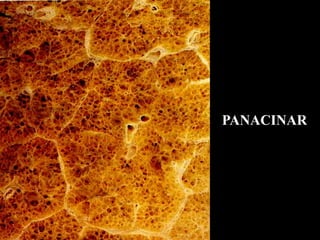
2. Panacinar
3. Paraseptal [Distal acinar]
4. Mixed & unclassified [Irregular]](https://image.slidesharecdn.com/emphysema-csbrp-130111113343-phpapp02/85/Emphysema-12-320.jpg)
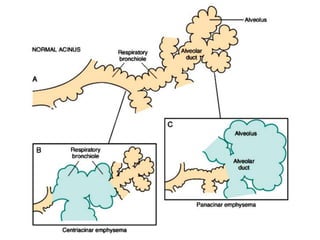
![Centriacinar :
[ centrilobular, Proximal acinar ]
• Dilatation of Respiratory Bronchiole
• Upper lobes - severely involved
• Can coexist with chronic bronchitis
• Invariably occurs in smokers
• Coal mine workers [carbon, dust]](https://image.slidesharecdn.com/emphysema-csbrp-130111113343-phpapp02/85/Emphysema-16-320.jpg)

![Mixed [CENTRIACINAR + PARASEPTAL]](https://image.slidesharecdn.com/emphysema-csbrp-130111113343-phpapp02/85/Emphysema-23-320.jpg)

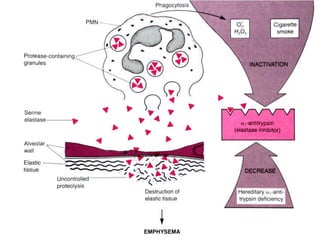
![Alpha-1 Antitrypsin deficiency
• 52 kD serum glycoprotein
• Synthesis: liver, macrophage
• Inhibits - Trypsin, Thrombin, Plasmin, Elastase
• Gene: chromosome 14 [75 alleles]
* Normal allele -- MM (90%)
* Deficiency -- ZZ](https://image.slidesharecdn.com/emphysema-csbrp-130111113343-phpapp02/85/Emphysema-30-320.jpg)
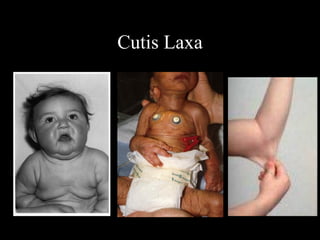
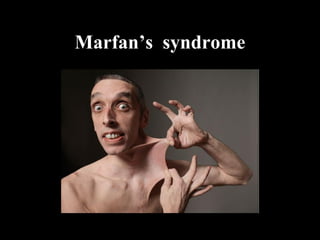
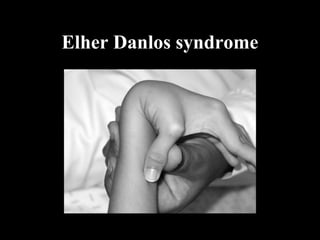
![Etiology
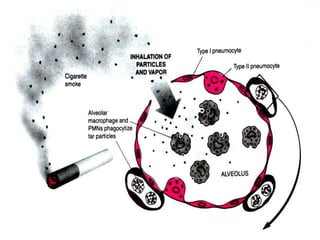
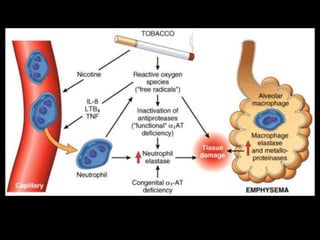
• Cigarette smoking [20 - 40% smokers]
• Air pollution
• Alpha-1-antitrypsin deficiency
• Inherited diseases ( Rare )
* Cutis laxa
* Marfan’s syndrome
* Menke’s syndrome](https://image.slidesharecdn.com/emphysema-csbrp-130111113343-phpapp02/85/Emphysema-33-320.jpg)
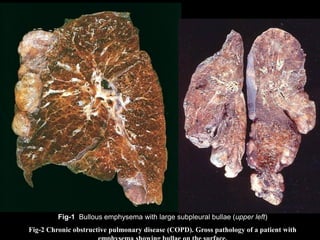
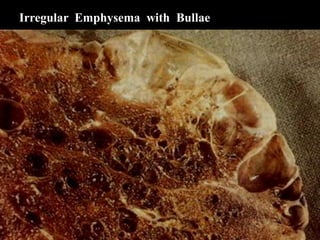

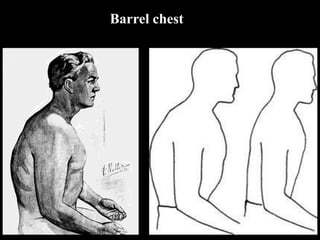
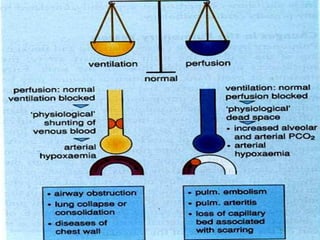
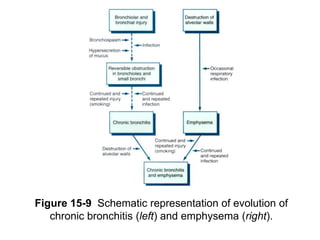
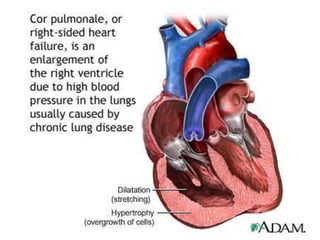
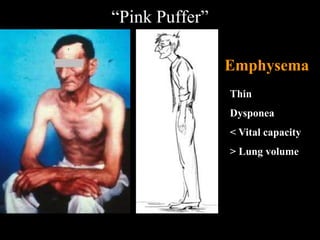
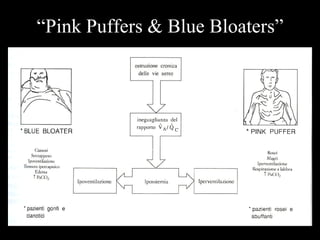
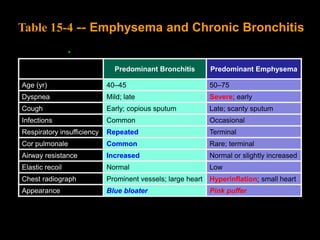

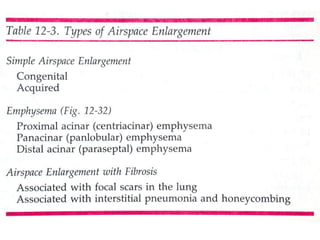
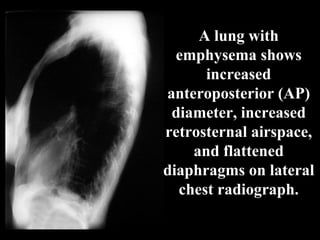
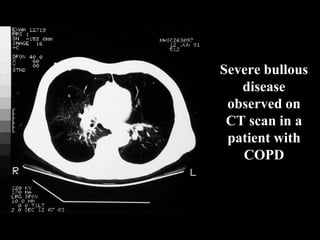
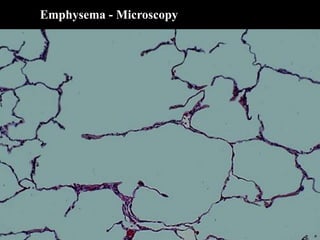
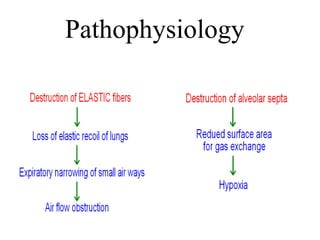
1. Emphysema is a chronic obstructive pulmonary disease characterized by abnormal enlargement of the airspaces in the lungs accompanied by destruction of their walls. 2. The main symptoms of emphysema include dyspnea, recurrent respiratory infections, and right heart failure. Chest imaging shows increased lung volumes and flattened diaphragms. 3. There are several classifications of emphysema based on the areas of the lung affected, including centriacinar, panacinar, paraseptal, and mixed emphysema. Cigarette smoking is a major risk factor and can cause an imbalance of proteases and antiproteases in the lungs.