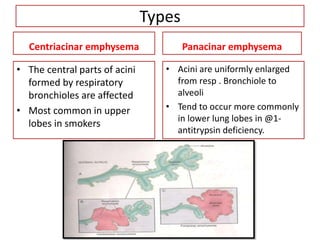
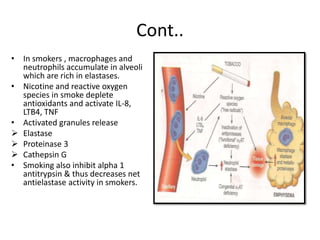
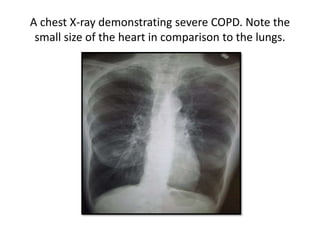
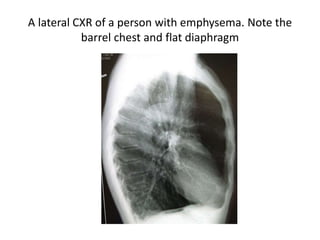
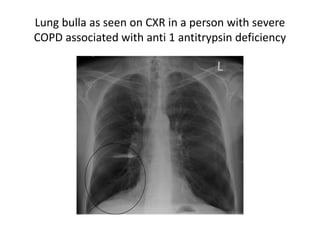
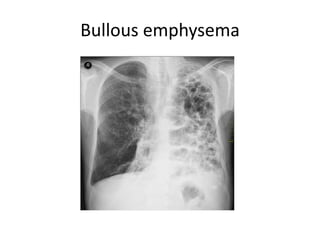
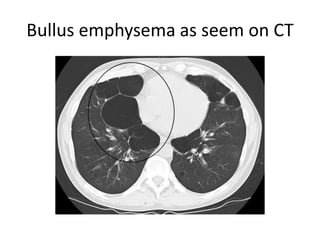
Emphysema is a lung disease characterized by abnormal enlargement of the air spaces in the lungs. There are several types of emphysema including centriacinar, panacinar, distal acinar, and irregular emphysema. The main pathogenesis involves an imbalance between protease enzymes like elastase released by smoke exposure and antioxidant proteins like alpha-1 antitrypsin that normally inhibit these enzymes. This imbalance leads to destruction of lung elastic tissue and enlargement of the air spaces. Patients may present as "pink puffers" with barrel chests and prolonged expiration or "blue bloaters" with hypoxia and cor pulmonale. Diagnosis involves spirometry showing reduced FEV1 and imaging