Downloaded 480 times











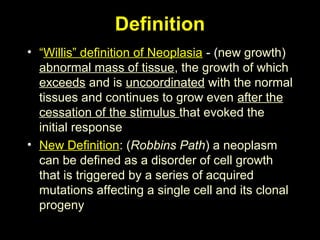
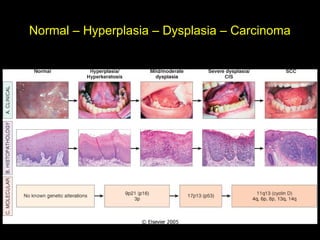

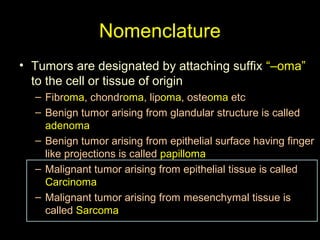
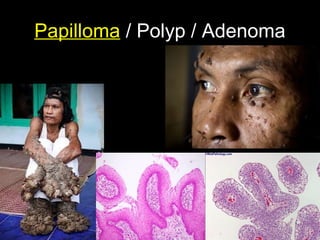
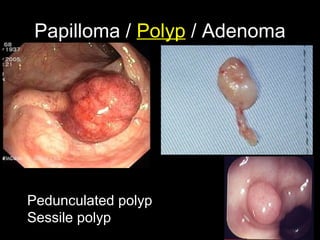
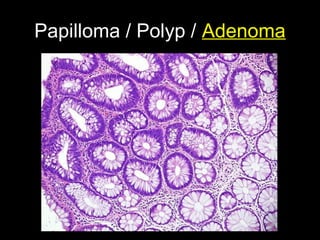
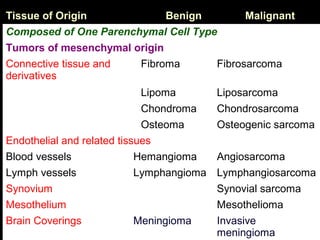
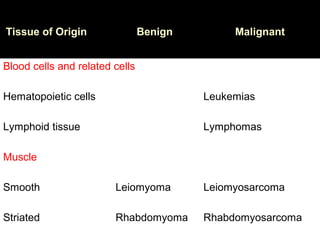
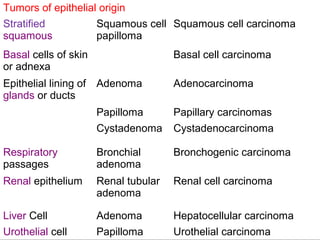
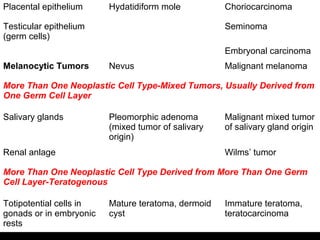
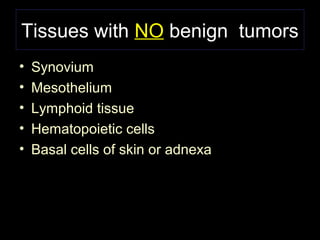
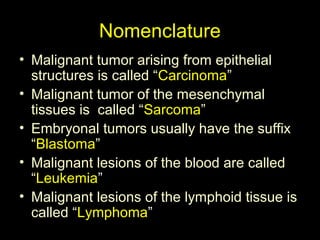
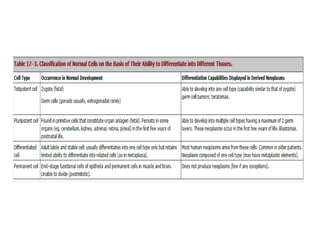
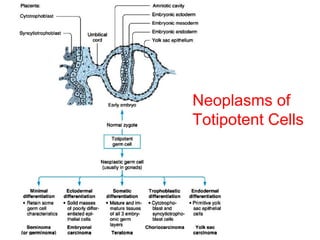
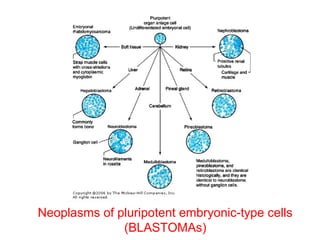
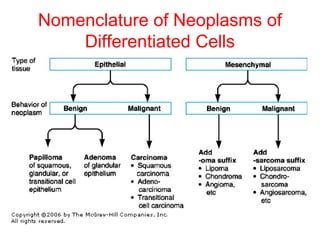


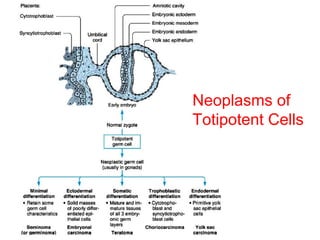
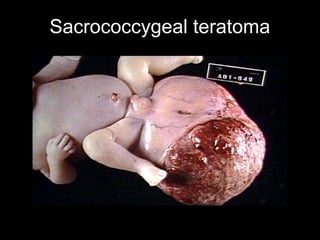

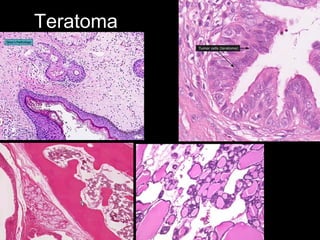
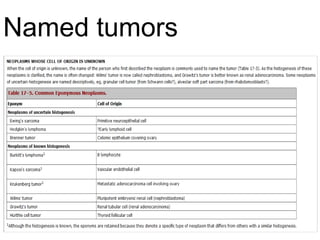
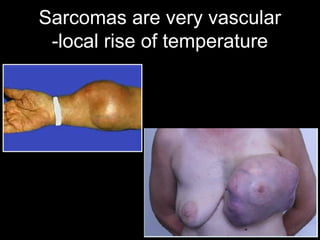
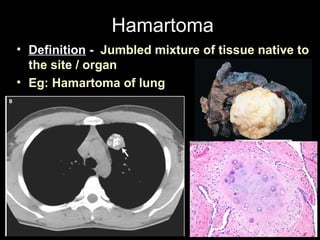
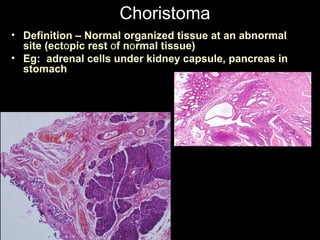
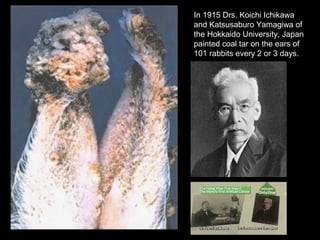


This document provides information on neoplasia (new growth) and tumor nomenclature. It defines neoplasia as abnormal and uncontrolled cell growth that exceeds normal tissues. Tumors are named based on their cell or tissue of origin, with benign tumors ending in "-oma" and malignant tumors called carcinomas for epithelial cells and sarcomas for mesenchymal cells. Common sites for teratomas are the gonads and along midline fusion lines. Hamartomas contain normal tissues for the organ, while choristomas contain ectopic tissues. Environmental exposures like coal tar were found to induce skin cancer in rabbits.




![Neoplasia [part 1]](https://cdn.slidesharecdn.com/ss_thumbnails/neoplasiapart1-190918152450-thumbnail.jpg?width=640&height=640&fit=bounds)




































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)













