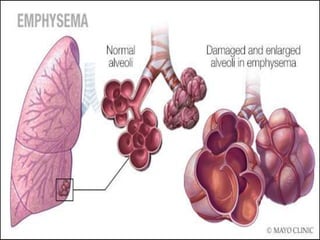
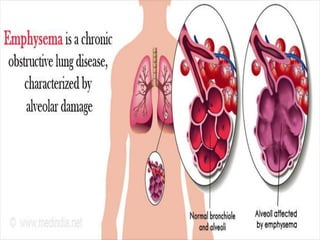
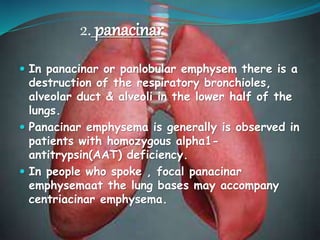
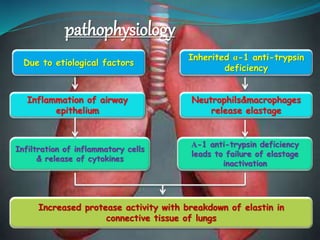
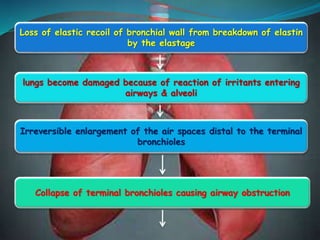
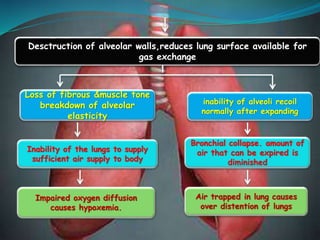
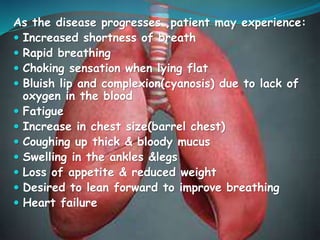
Emphysema is a lung disease that causes damage to the air sacs in the lungs called alveoli, resulting in shortness of breath. It is usually caused by smoking or long-term exposure to irritants or pollutants. As the disease progresses, the alveoli are destroyed, reducing the lungs' ability to take in oxygen. Symptoms start mild but worsen over time, ultimately causing severe shortness of breath and respiratory failure if left untreated. Treatment focuses on quitting smoking, medications, surgery, pulmonary rehabilitation, and managing symptoms.