
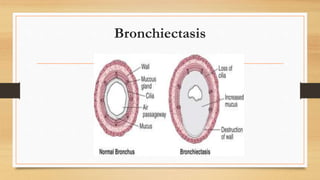





Bronchiectasis is a chronic lung condition characterized by abnormal dilation of the bronchi. It can be caused by airway obstruction, pulmonary infections, genetic disorders like cystic fibrosis, or idiopathic factors. Symptoms include persistent cough with large amounts of sputum, hemoptysis, and clubbing of the fingers. Diagnosis is made through chest imaging like HRCT. Treatment focuses on clearing secretions through postural drainage, chest physiotherapy, antibiotics, bronchodilators, and smoking cessation. Nursing management centers on helping patients perform breathing exercises and techniques to clear pulmonary secretions.








































































































