Downloaded 82 times



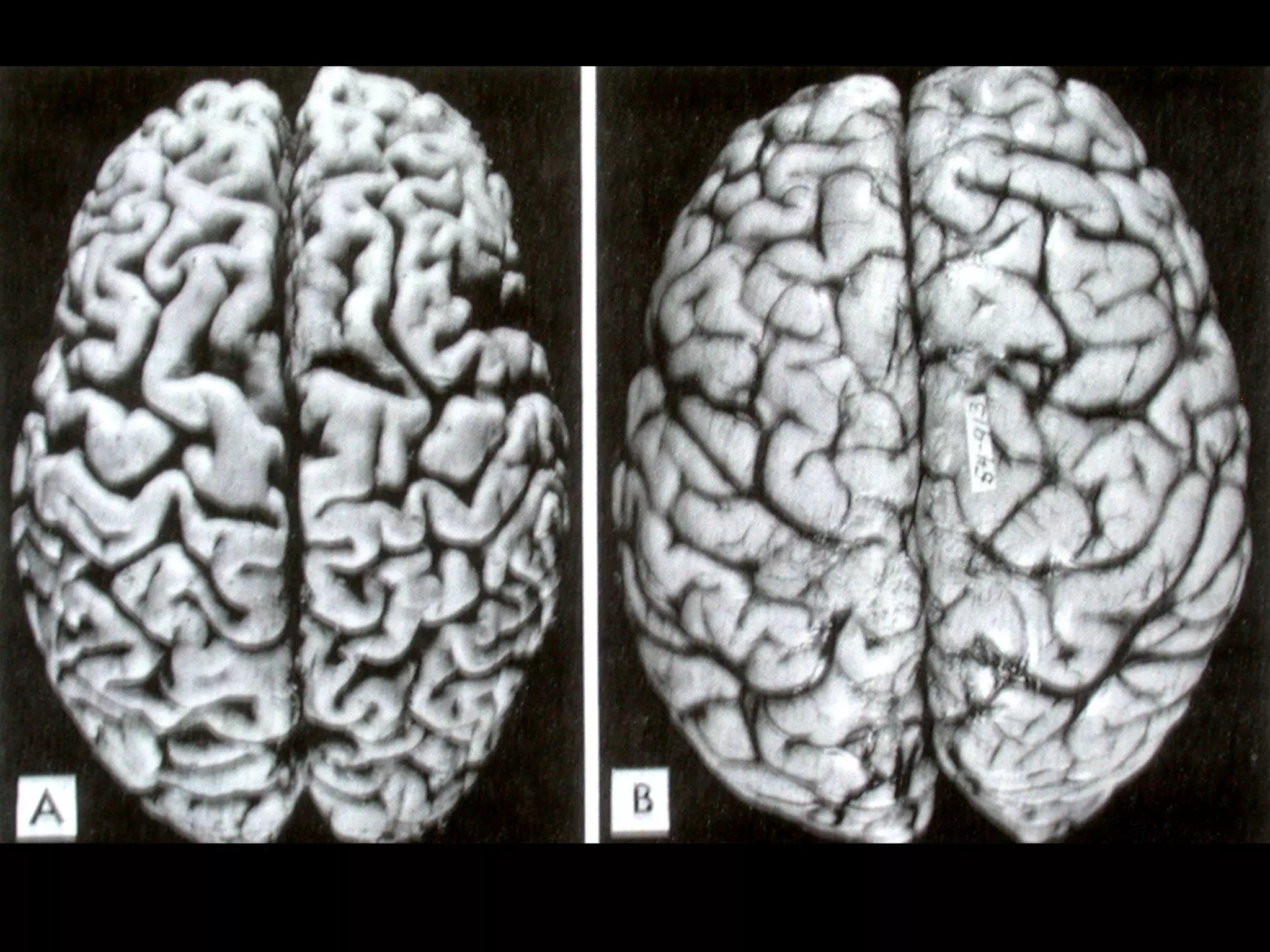





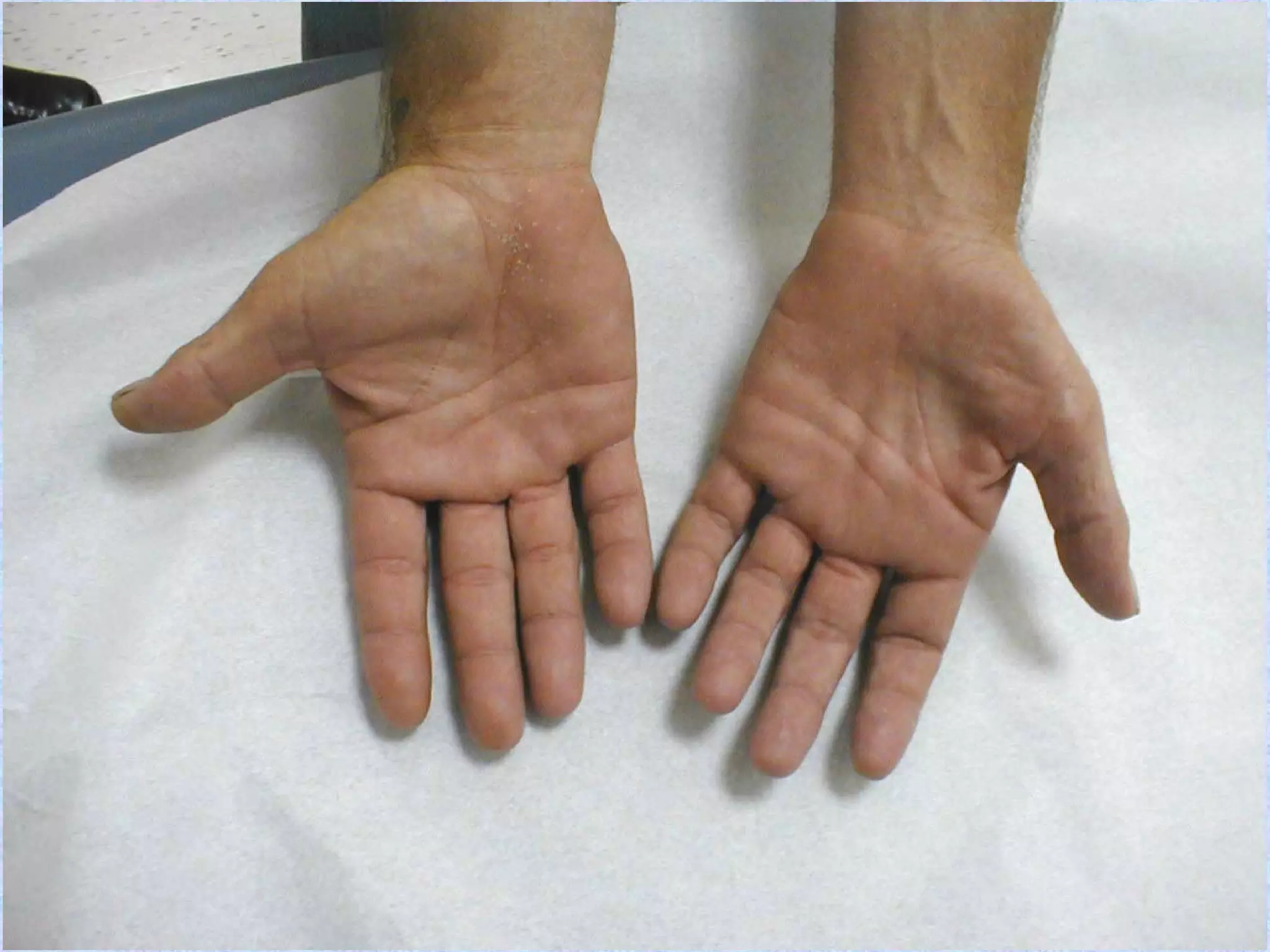














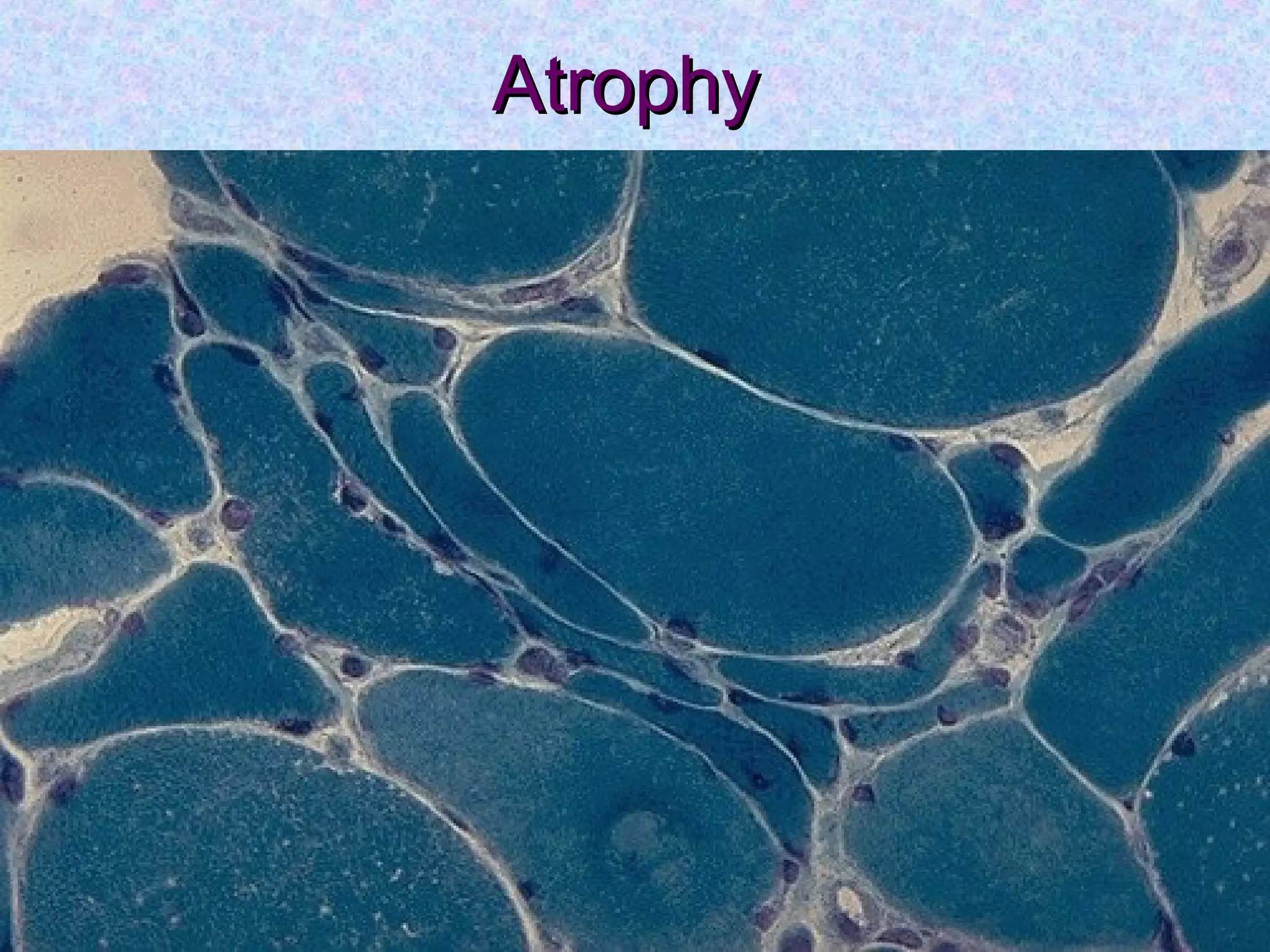





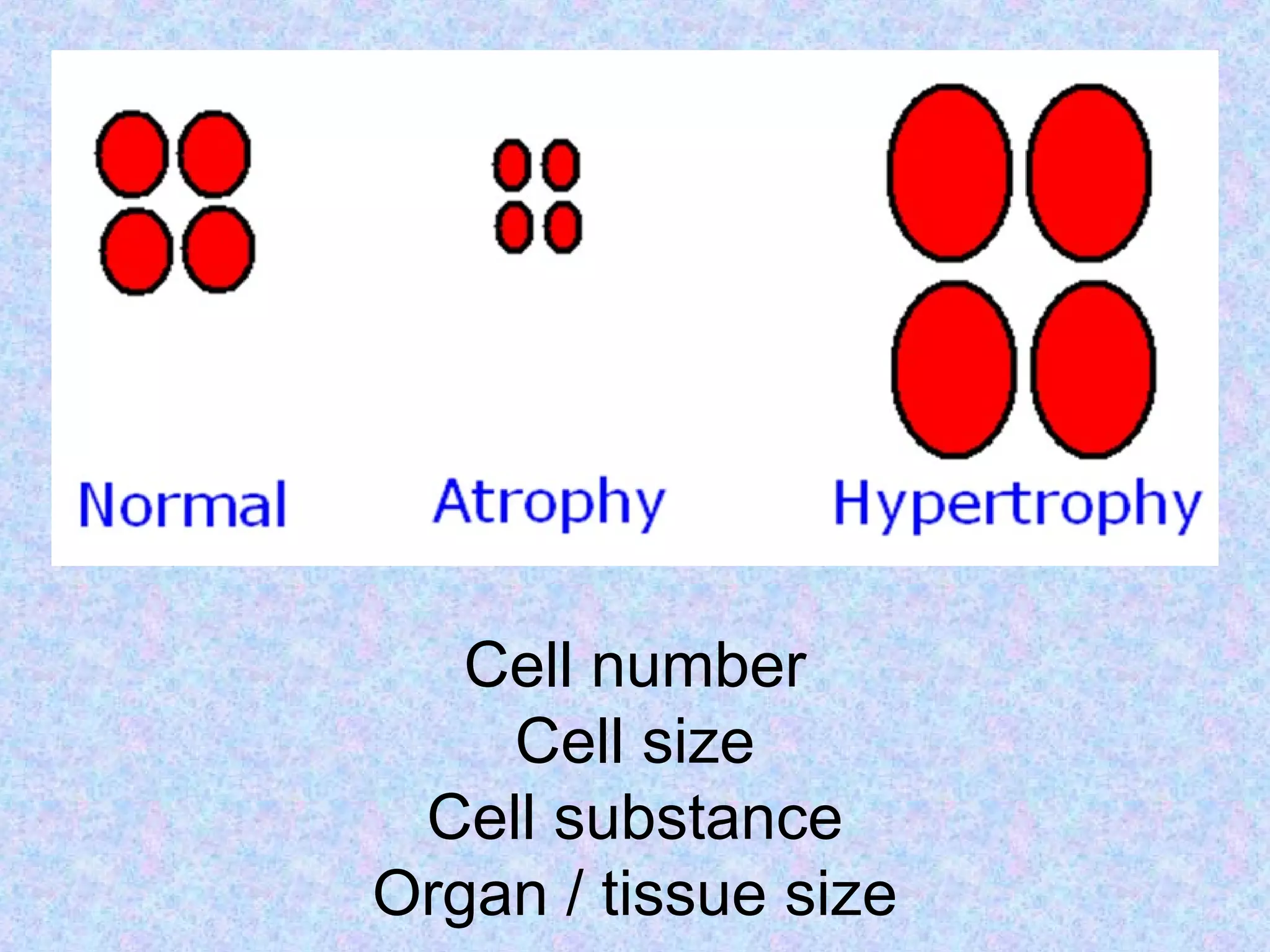








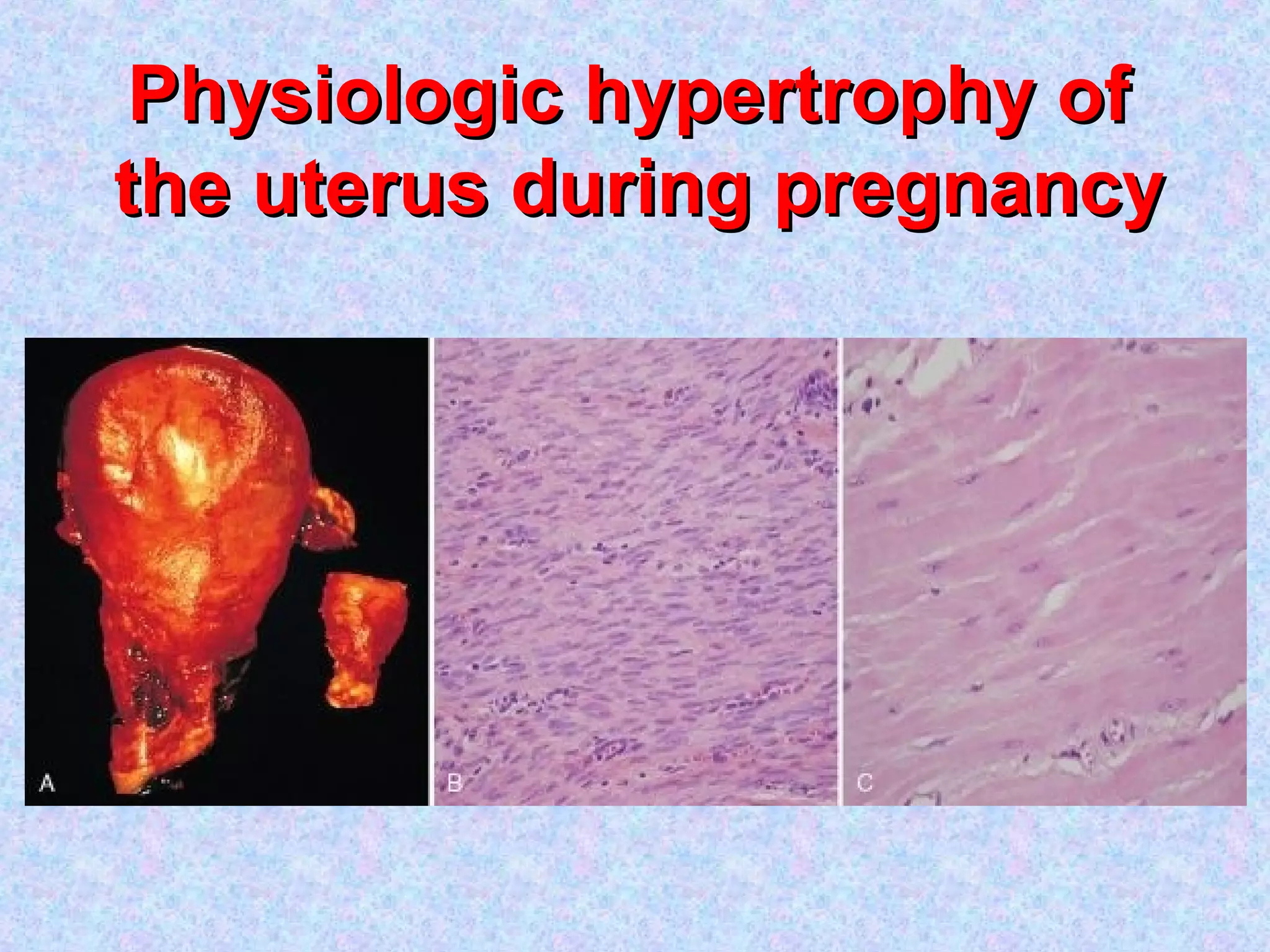











































Atrophy is the shrinkage of cells and tissues due to loss of cellular components. It can result from decreased workload, blood supply, nutrition, endocrine stimulation or aging. At the microscopic level, atrophied cells appear smaller with more autophagic vacuoles and lipofuscin accumulation. Cancer cachexia involves activation of the proteasome pathway leading to muscle wasting. Hypertrophy is the enlargement of cells and tissues due to an increase in cellular components but without an increase in cell number. It can be physiological such as in pregnancy or pathological such as in response to hypertension. The mechanisms involve increased protein synthesis, DNA content or cellular phenotype. Over time, degenerative changes can occur.

































































































