
![Classification: Types of emphysema
1. Centriacinar
2. Panacinar
3. Paraseptal [Distal acinar]
4. Mixed & unclassified [Irregular]](https://image.slidesharecdn.com/13-220901180723-aff3f523/75/13-Emphysema-pptx-5-2048.jpg)
![Centriacinar :
[ centrilobular, Proximal acinar ]
• Dilatation of Respiratory Bronchiole
• Upper lobes - severely involved
• Can coexist with chronic bronchitis
• Invariably occurs in smokers
• Coal mine workers [carbon, dust]](https://image.slidesharecdn.com/13-220901180723-aff3f523/75/13-Emphysema-pptx-6-2048.jpg)


![Etiology
• Cigarette smoking [20 - 40% smokers]
• Air pollution
• Alpha-1-antitrypsin deficiency](https://image.slidesharecdn.com/13-220901180723-aff3f523/75/13-Emphysema-pptx-10-2048.jpg)


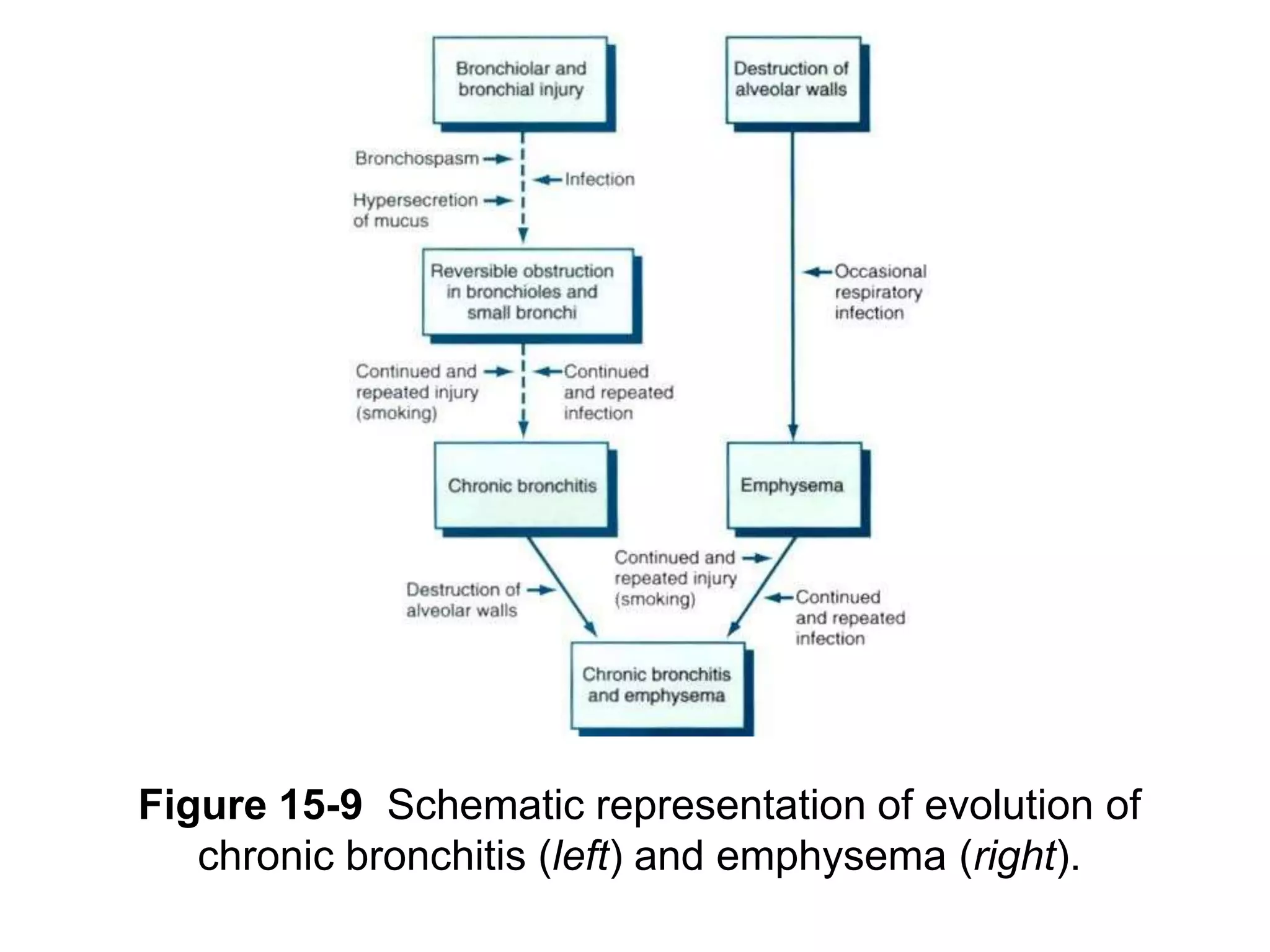






Emphysema is a chronic lung disease characterized by abnormal enlargement of the airspaces in the lungs. It is caused by destruction of the walls of the alveoli, the tiny air sacs in the lungs. There are several types of emphysema including centriacinar, panacinar, and paraseptal. The main symptoms of emphysema include shortness of breath, cough, and wheezing. Smoking is the leading cause of emphysema and it can also be caused by air pollution and genetic conditions like alpha-1 antitrypsin deficiency. Emphysema is a component of chronic obstructive pulmonary disease (COPD) along with chronic bronchitis,