Downloaded 6,649 times
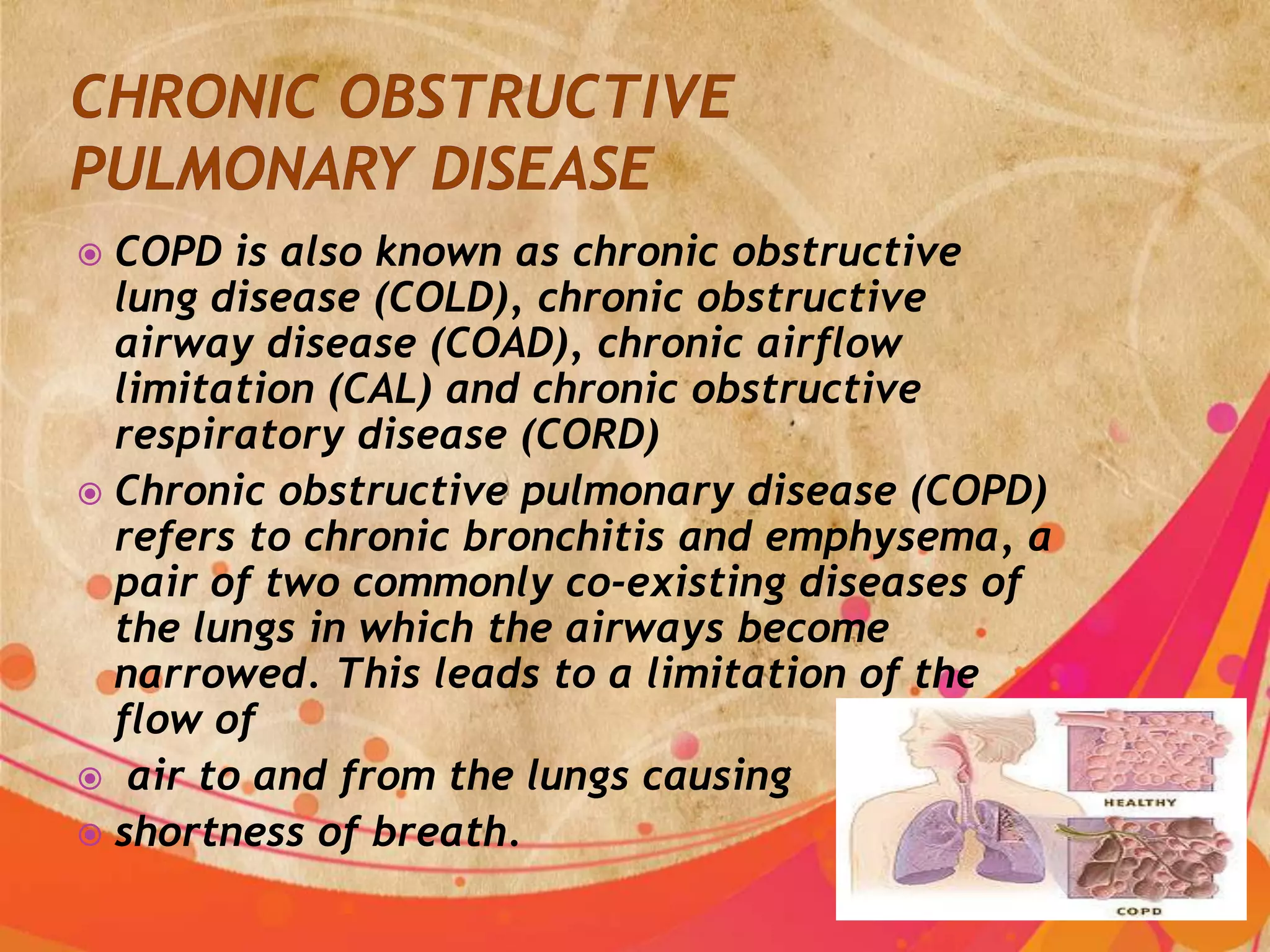
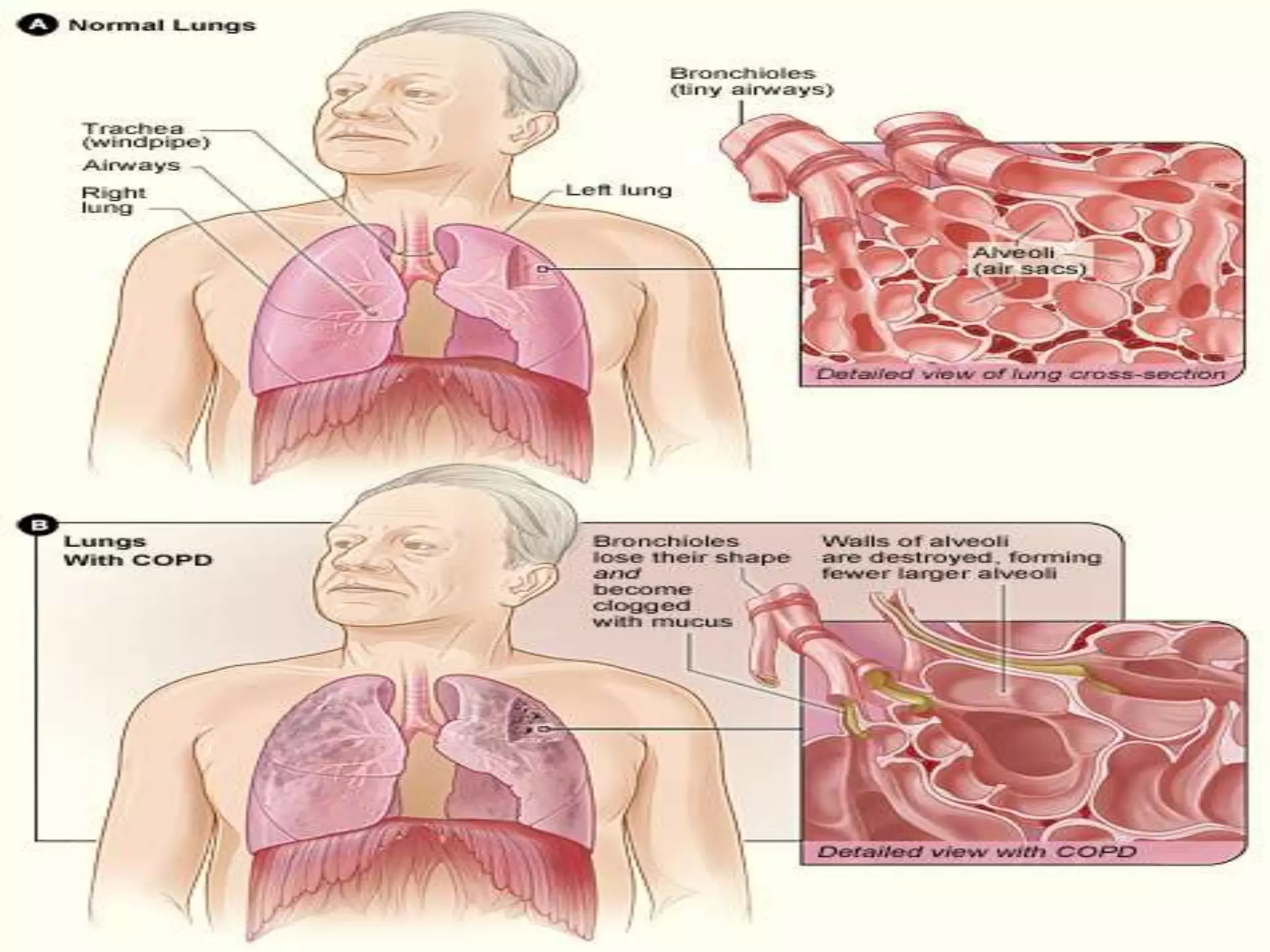
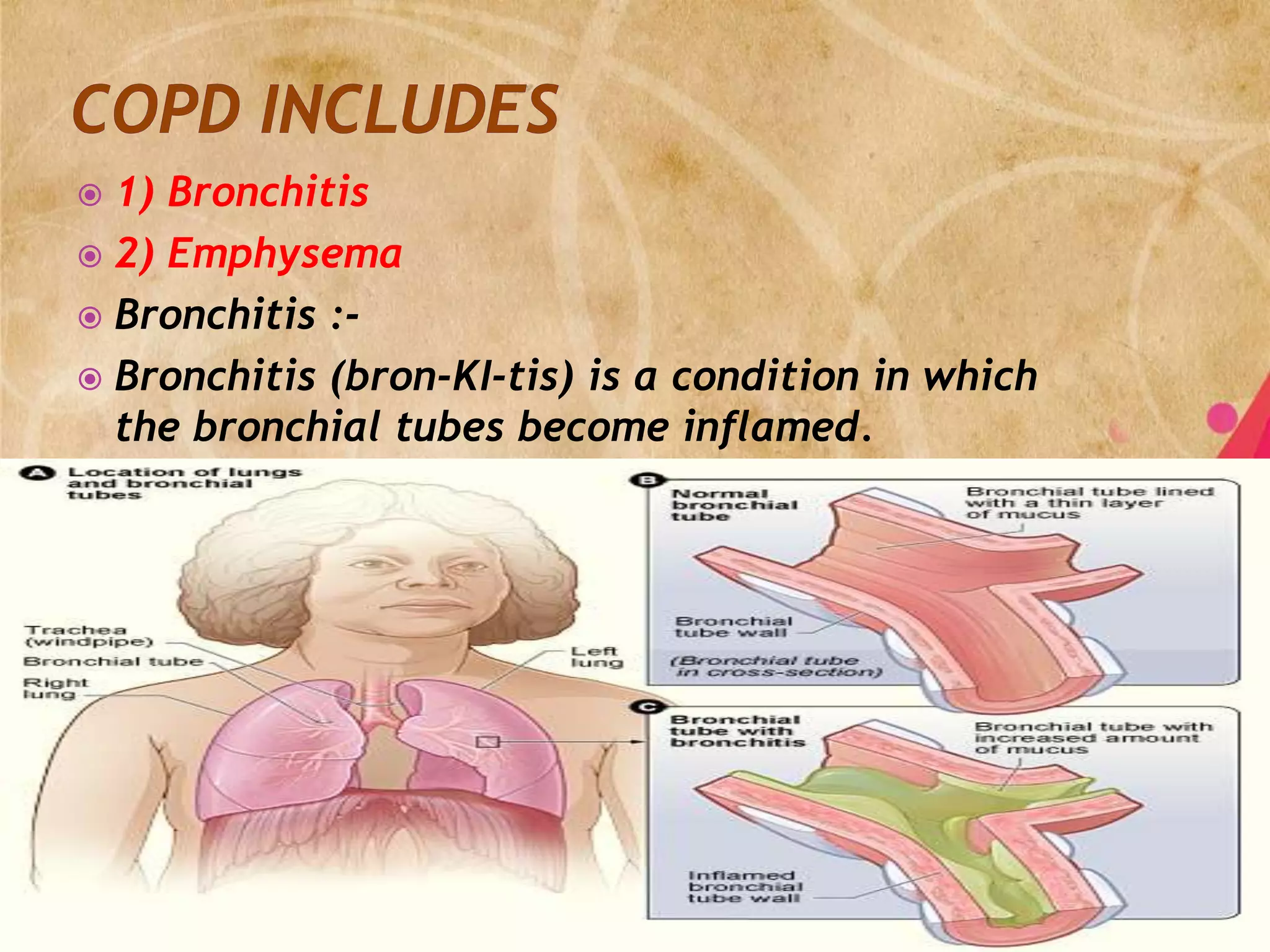
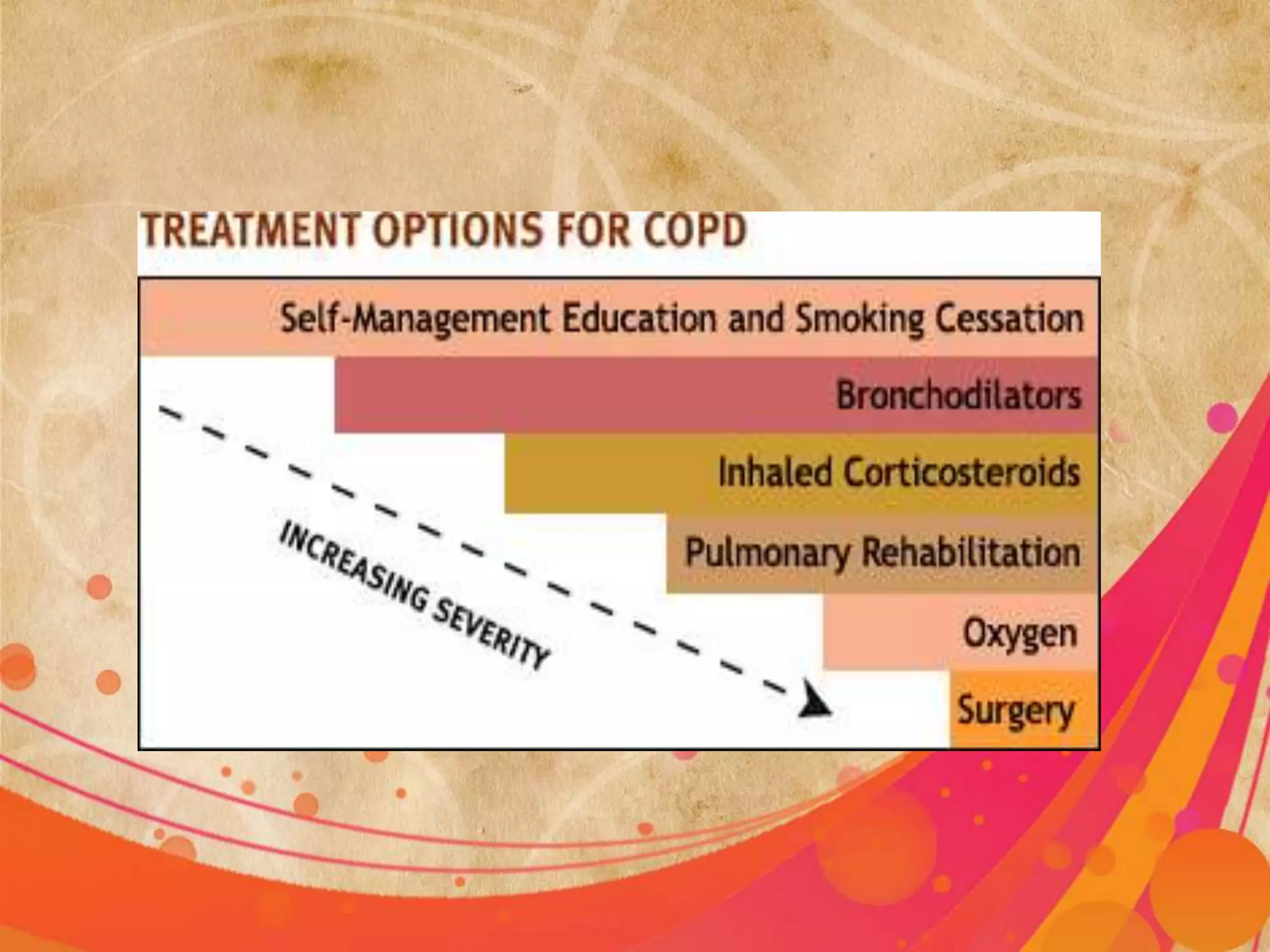





Chronic obstructive pulmonary disease (COPD) refers to two lung diseases, chronic bronchitis and emphysema, that are typically caused by smoking and result in limited airflow. The document discusses the definition, causes, symptoms, diagnosis, and management of COPD. It notes that COPD is the 4th leading cause of death and involves inflammation and narrowing of the airways leading to shortness of breath. Treatment focuses on improving ventilation, removing secretions, managing complications, and improving overall health.























































































