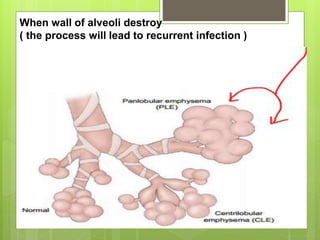
Emphysema is damage and abnormal distention of airspaces beyond the terminal bronchioles caused by cigarette smoking or air pollution. There are four main types: centrilobular affects central acini, panlobular affects all acini uniformly, distal acinar involves distal parts of acini, and irregular is mixed. Symptoms include shortness of breath, cough, difficulty breathing with exertion, and barrel chest. Complications can include respiratory failure, pneumonia, pulmonary hypertension, and right heart failure. Treatment involves smoking cessation, bronchodilators, oxygen therapy, and possibly surgery. Nursing care focuses on monitoring vital signs, administering medications and oxygen, and maintaining proper positioning.