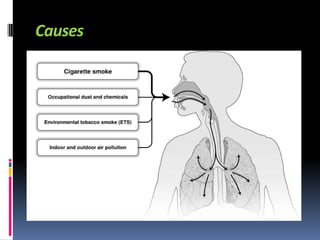
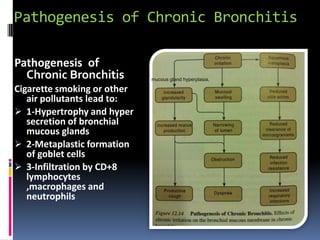
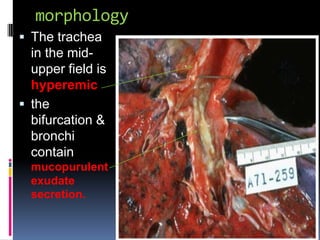
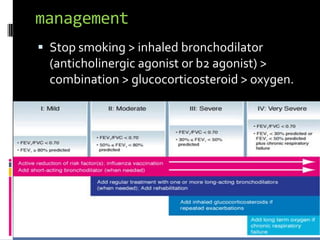
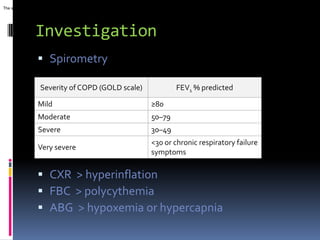
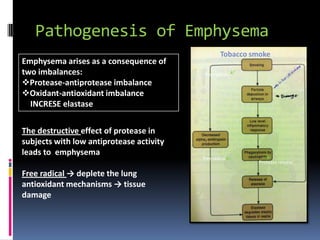
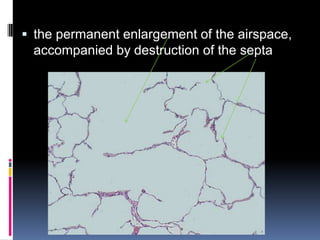
The document discusses chronic bronchitis, emphysema, and pulmonary hypertension. It defines each condition and describes their causes, pathophysiology, morphology, management, complications, symptoms, and methods of investigation including spirometry and chest x-rays. Chronic bronchitis involves inflammation of the bronchi due to smoking or air pollution. Emphysema is the permanent enlargement of airspaces due to an imbalance of proteases and antioxidants from smoking. Pulmonary hypertension is high blood pressure in the lungs secondary to lung damage from these conditions.