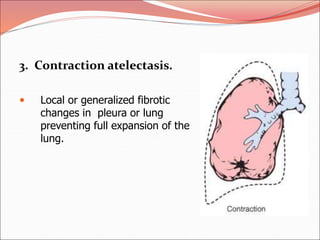
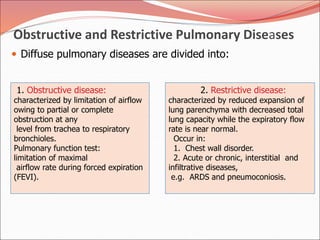
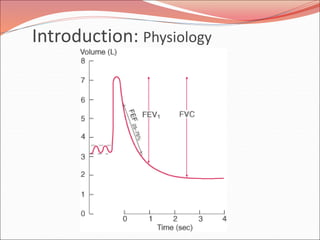
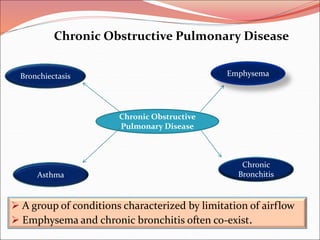
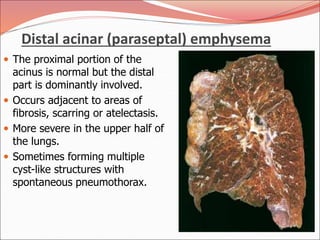
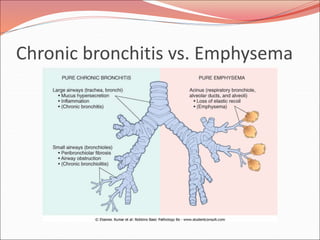
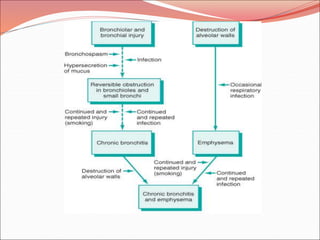
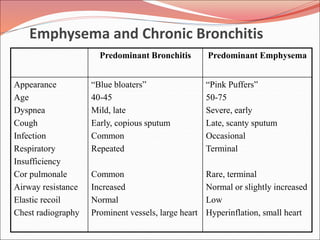
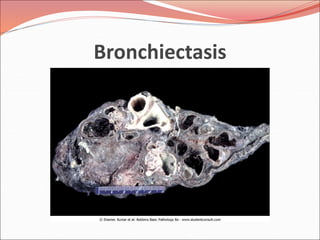
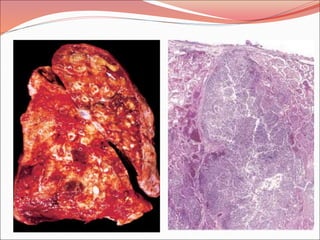
The document discusses several lung diseases including obstructive lung diseases, restrictive pulmonary diseases, pulmonary infections, lung tumors, and diseases of the pleura. It provides details on specific conditions such as atelectasis, chronic obstructive pulmonary disease (COPD), emphysema, chronic bronchitis, asthma, and bronchiectasis. For each condition, it describes the pathogenesis, clinical presentation, morphology, and clinical course. It also compares and contrasts emphysema and chronic bronchitis.
































































![BIOMEDICAL_WASTE_MANAGEMENT[1].pptx 22222.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/biomedicalwastemanagement1-240420050706-3b1ae262-thumbnail.jpg?width=640&height=640&fit=bounds)
























