Downloaded 501 times
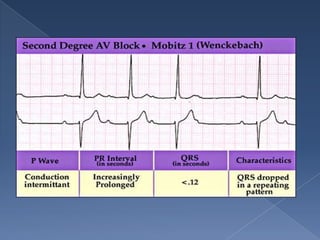

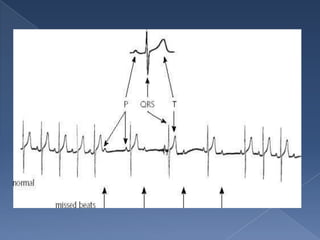


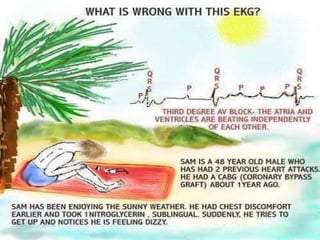


This document discusses different types of heart block. Second degree heart block involves intermittent conduction of electrical impulses from the atria to the ventricles. Mobitz type I (Wenckebach) involves progressive lengthening of the PR interval followed by a blocked beat, while Mobitz type II involves sudden blocked beats without PR prolongation. Third degree heart block occurs when there is complete absence of conduction between the atria and ventricles. Treatment depends on the severity and type of heart block, ranging from monitoring to pacemaker implantation.

![Acute heart failure [MBBS]](https://cdn.slidesharecdn.com/ss_thumbnails/acuteheartfailure-170323061012-thumbnail.jpg?width=640&height=640&fit=bounds)






























![ECG & Heart block [doctors online]](https://cdn.slidesharecdn.com/ss_thumbnails/ecgheartblockdoctorsonline-131111054313-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)










































































