Downloaded 2,271 times























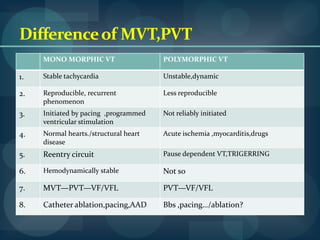







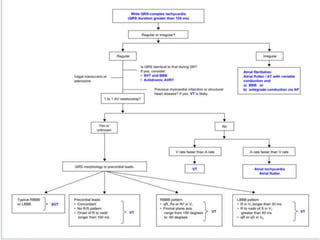
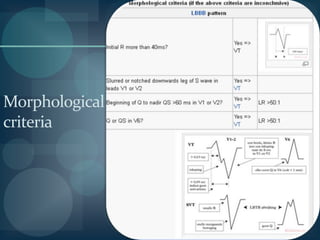




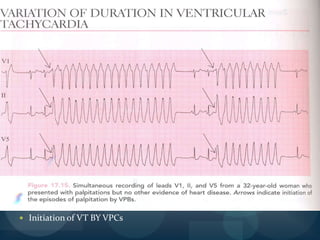







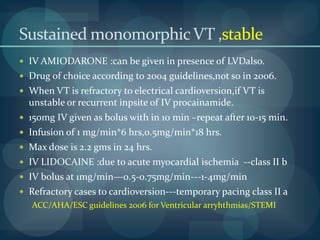







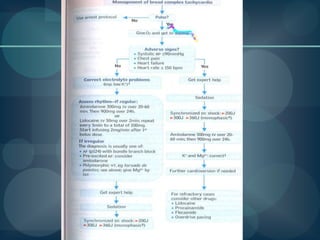




























Ventricular tachycardia can occur due to various causes like acute myocardial infarction, chronic infarction, dilated cardiomyopathy, etc. It is classified as sustained, non-sustained, monomorphic, polymorphic, etc. based on characteristics. Diagnosis involves ECG, echocardiogram, and monitoring. Treatment depends on hemodynamic stability and includes electrical cardioversion, antiarrhythmic drugs like amiodarone, lidocaine, ablation, and ICD implantation in selected cases. Recurrence risk is high in structurally abnormal hearts and prevention involves controlling triggers, antiarrhythmics, and ICDs.











































































































