Downloaded 663 times



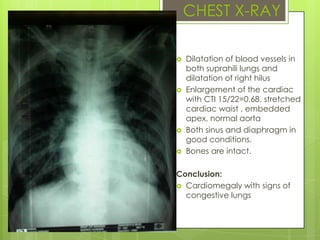





























Mr. I, a 64-year-old male, presented to the hospital with chest pain. He reported feeling pressure and tightness in his chest for the past 5 months that had worsened. Examinations found elevated blood pressure, tachycardia, and signs of cardiomegaly on chest x-ray. ECG showed sinus rhythm with poor R wave progression. Echocardiogram indicated left ventricular dysfunction. The working diagnosis was unstable angina pectoris and hypertension. Management included medications to reduce blood pressure and prevent clots, with monitoring through daily ECGs.








































































![[FAR] Faradhillah A. Suryadi - Pemeriksaan Refraksi Objektif - cor.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/farfaradhillaha-230306165042-75bda47d-thumbnail.jpg?width=640&height=640&fit=bounds)


































