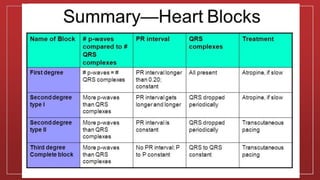
Heart block occurs when the electrical signals that tell the heart to contract are partially or totally blocked between the atria and ventricles, causing the heart to beat too slowly. There are three main types of heart block - first degree, second degree, and third degree (complete heart block). The type of heart block depends on how much the electrical signals are blocked. More advanced heart blocks require treatment such as pacemakers while milder forms often do not require treatment.
























































![Shadechapter12.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter12-150421103821-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)












































