Downloaded 103 times
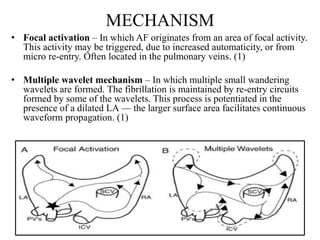

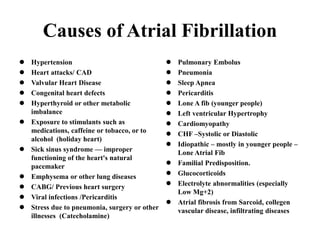
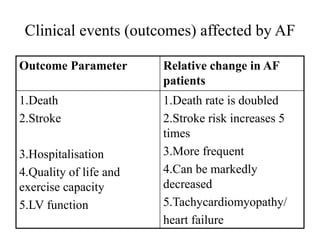
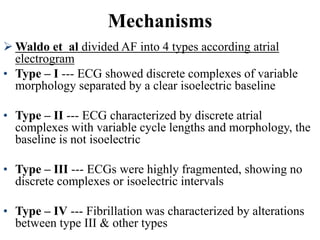
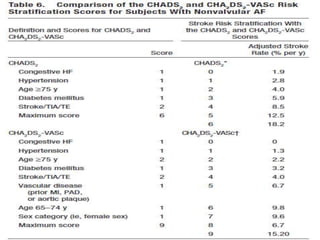
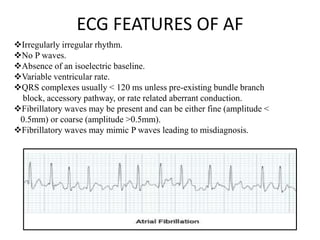
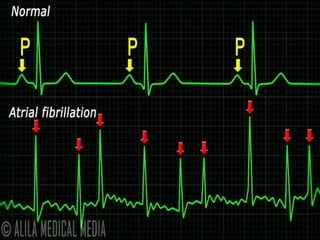
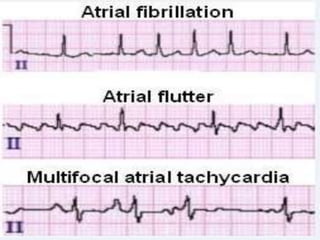
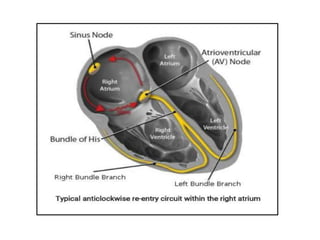
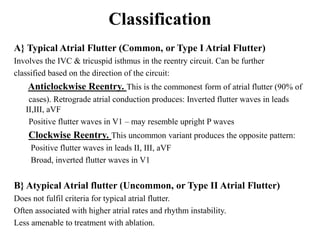
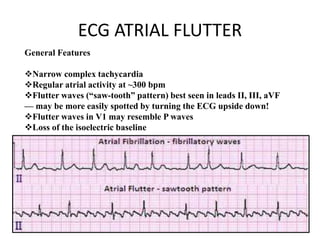


This document provides an overview of atrial fibrillation (AF) and atrial flutter. It discusses the characteristics, mechanisms, ECG features, causes and clinical outcomes of AF. It also covers the classification, mechanisms, ECG patterns and examples of atrial flutter. Key points include that AF is characterized by disorganized atrial activation and irregular ventricular rhythm, while flutter involves a reentrant circuit in the right atrium causing a regular atrial rate of 300 bpm. Complications of AF include increased risk of stroke, heart failure and cardiac death.