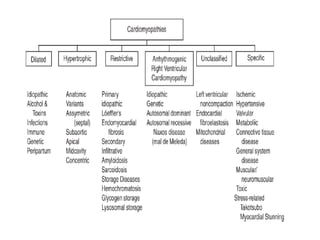
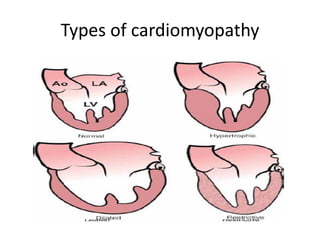
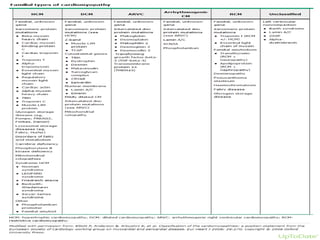
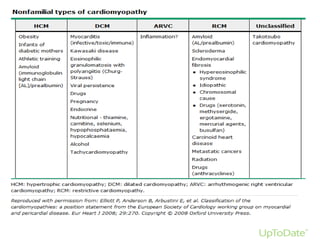
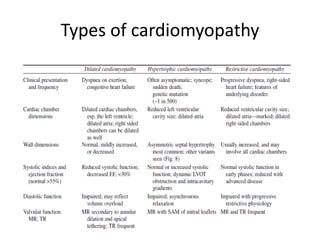
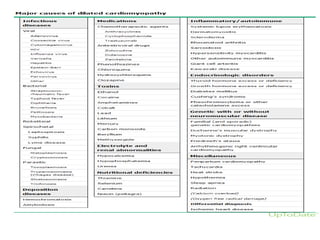
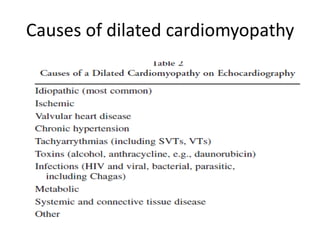
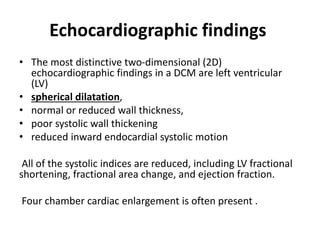
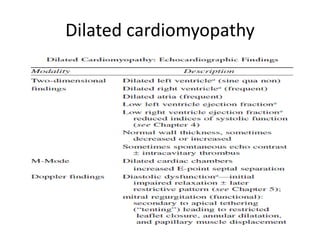
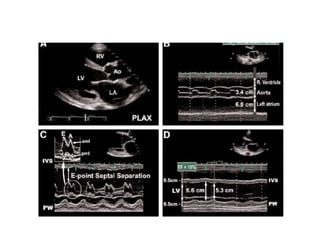
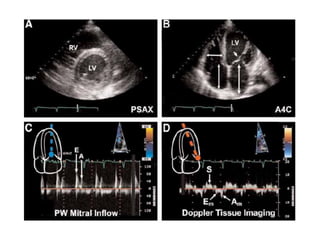
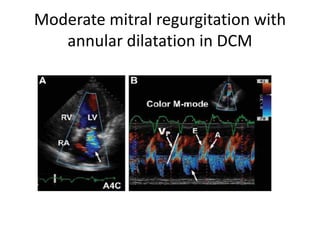
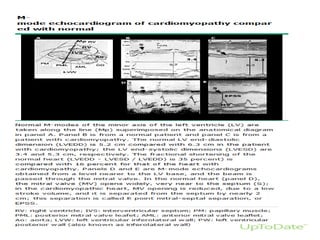
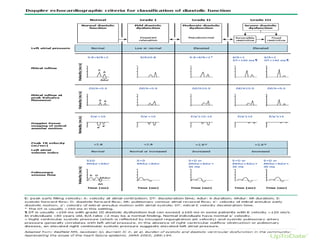
This document discusses the echocardiographic evaluation of cardiomyopathies. It defines cardiomyopathy and outlines the major classification systems. The main types discussed are dilated cardiomyopathy, hypertrophic cardiomyopathy, arrhythmogenic right ventricular cardiomyopathy, restrictive cardiomyopathy, and unclassified cardiomyopathy. Specific features of dilated cardiomyopathy are then reviewed in detail, including morphological features, causes, Doppler findings, and involvement of the right ventricle and left atrium. Evaluation of diastolic dysfunction and ischemic cardiomyopathy are also summarized.




































































![Myocardial infarction [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/myocardialinfarctionautosaved-210125122422-thumbnail.jpg?width=640&height=640&fit=bounds)



![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)










![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




