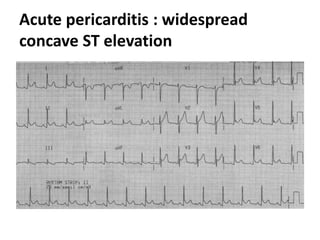
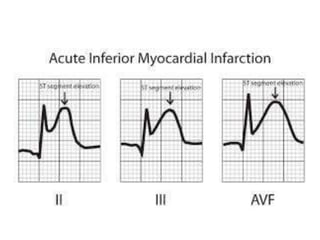
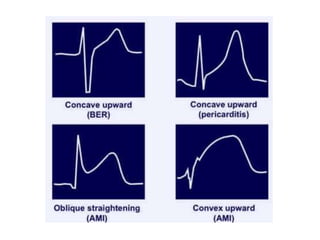
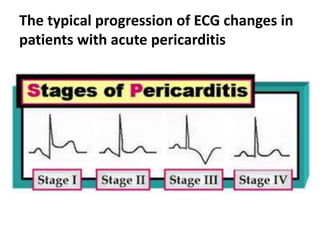
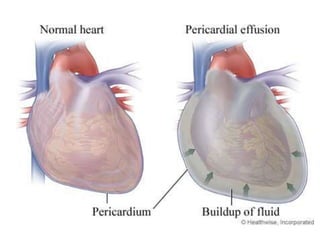
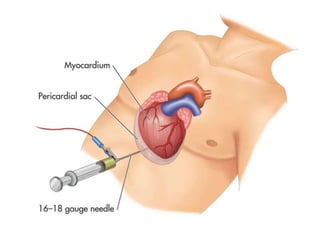
The document discusses acute pericarditis, which is the most common disorder of the pericardium. The pericardium is a sac surrounding the heart. Acute pericarditis can be caused by infections, cardiac issues, autoimmune diseases, metabolic problems, neoplasms, drugs, or trauma. Common symptoms include chest pain, a pericardial friction rub sound, and ECG changes showing widespread concave ST elevation. Treatment typically involves NSAIDs and colchicine, though some cases require invasive therapies like drainage. Prognosis is generally good, but risks include cardiac tamponade or constrictive pericarditis.