TABLE OF CONTENTS
Whatis Heart Block?
Normal Cardiac Conduction Review
Causes and Risk Factors
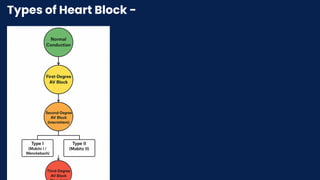
Types of Heart Block:
First-Degree AV Block
Second-Degree AV Block (Mobitz Type I & II)
Third-Degree (Complete) AV Block
Symptoms
Diagnosis
Management & Treatment
Complications
3.
INTRODUCTION
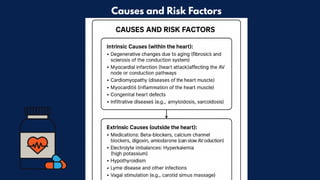
Definition: Heart block(or atrioventricular (AV)
block) is a condition where the electrical signals
that tell your heart to beat are either delayed or
completely blocked from reaching the ventricles.
4.
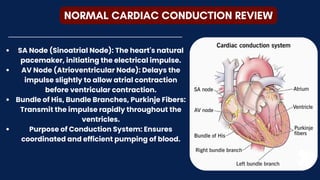
NORMAL CARDIAC CONDUCTIONREVIEW
SA Node (Sinoatrial Node): The heart's natural
pacemaker, initiating the electrical impulse.
AV Node (Atrioventricular Node): Delays the
impulse slightly to allow atrial contraction
before ventricular contraction.
Bundle of His, Bundle Branches, Purkinje Fibers:
Transmit the impulse rapidly throughout the
ventricles.
Purpose of Conduction System: Ensures
coordinated and efficient pumping of blood.
The heart wallis composed of three layers:
Epicardium: The outer protective layer.
Myocardium: The muscular middle layer responsible
for contraction.
Endocardium: The inner lining that contacts the
blood.
The Septum: The septum is a muscular wall that
divides the heart into left and right sides, preventing
the mixing of oxygen-rich and oxygen-poor blood.
WALLS OF THE HEART
7.
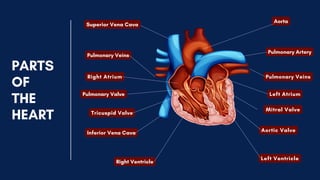
STRUCTURE OF THEHEART
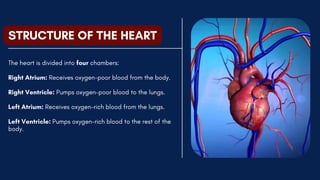
The heart is divided into four chambers:
Right Atrium: Receives oxygen-poor blood from the body.
Right Ventricle: Pumps oxygen-poor blood to the lungs.
Left Atrium: Receives oxygen-rich blood from the lungs.
Left Ventricle: Pumps oxygen-rich blood to the rest of the
body.
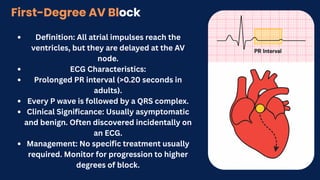
Definition: All atrialimpulses reach the
ventricles, but they are delayed at the AV
node.
ECG Characteristics:
Prolonged PR interval (>0.20 seconds in
adults).
Every P wave is followed by a QRS complex.
Clinical Significance: Usually asymptomatic
and benign. Often discovered incidentally on
an ECG.
Management: No specific treatment usually
required. Monitor for progression to higher
degrees of block.
First-Degree AV Block
11.
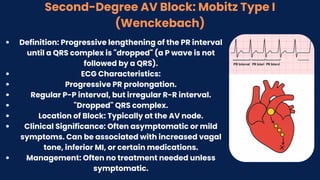
Second-Degree AV Block:Mobitz Type I
(Wenckebach)
Definition: Progressive lengthening of the PR interval
until a QRS complex is "dropped" (a P wave is not
followed by a QRS).
ECG Characteristics:
Progressive PR prolongation.
Regular P-P interval, but irregular R-R interval.
"Dropped" QRS complex.
Location of Block: Typically at the AV node.
Clinical Significance: Often asymptomatic or mild
symptoms. Can be associated with increased vagal
tone, inferior MI, or certain medications.
Management: Often no treatment needed unless
symptomatic.
12.
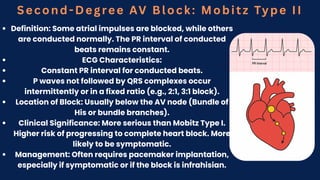
Second-Degree AV Block:Mobitz Type II
Definition: Some atrial impulses are blocked, while others
are conducted normally. The PR interval of conducted
beats remains constant.
ECG Characteristics:
Constant PR interval for conducted beats.
P waves not followed by QRS complexes occur
intermittently or in a fixed ratio (e.g., 2:1, 3:1 block).
Location of Block: Usually below the AV node (Bundle of
His or bundle branches).
Clinical Significance: More serious than Mobitz Type I.
Higher risk of progressing to complete heart block. More
likely to be symptomatic.
Management: Often requires pacemaker implantation,
especially if symptomatic or if the block is infrahisian.
13.
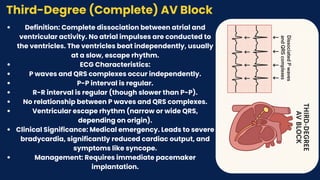
Third-Degree (Complete) AVBlock
Definition: Complete dissociation between atrial and
ventricular activity. No atrial impulses are conducted to
the ventricles. The ventricles beat independently, usually
at a slow, escape rhythm.
ECG Characteristics:
P waves and QRS complexes occur independently.
P-P interval is regular.
R-R interval is regular (though slower than P-P).
No relationship between P waves and QRS complexes.
Ventricular escape rhythm (narrow or wide QRS,
depending on origin).
Clinical Significance: Medical emergency. Leads to severe
bradycardia, significantly reduced cardiac output, and
symptoms like syncope.
Management: Requires immediate pacemaker
implantation.
14.
Symptoms of HeartBlock
Often depend on the degree of block and heart
rate.
Mild/Asymptomatic (First-degree, some Mobitz
I): May have no noticeable symptoms.
Moderate/Severe Symptoms (Mobitz II, Third-
degree):
Fatigue
Dizziness or lightheadedness
Syncope (fainting) or near-syncope
Shortness of breath, especially with exertion
Chest pain (angina)
Palpitations (awareness of slow heart beat)
Confusion
15.
Diagnosis
Medical History &Physical Examination: Assessing
symptoms, medical conditions, and medications.
Electrocardiogram (ECG/EKG): The primary diagnostic
tool. Reveals the specific type and degree of heart block.
Holter Monitor (Ambulatory ECG): 24-48 hour continuous
ECG recording to capture intermittent blocks.
Event Monitor: Worn for weeks or months to record rare,
symptomatic events.
Electrophysiology (EP) Study: Invasive procedure to
pinpoint the exact location and mechanism of the block,
especially in complex cases.
Blood Tests: To check for underlying causes (e.g.,
electrolytes, thyroid function, Lyme titers).
16.
Management & Treatment
Observation:For asymptomatic First-Degree and some
Mobitz Type I blocks.
Medication Review: Discontinue or adjust medications that
might be contributing to the block (e.g., beta-blockers,
calcium channel blockers).
Treating Underlying Causes: Address any reversible
conditions like electrolyte imbalances, hypothyroidism, or
infections.
Pacemaker Implantation:
Temporary Pacemaker: Used in acute situations (e.g.,
immediately after an MI with symptomatic block).
Permanent Pacemaker: The definitive treatment for
symptomatic Mobitz Type II and Third-Degree AV blocks. A
small device implanted under the skin, with wires leading to
the heart, to provide electrical impulses.
17.
Progression to higherdegrees of heart
block (e.g., Mobitz I to Mobitz II or Third-
degree).
Cardiac arrest (in severe cases of
third-degree block).
Heart failure due to prolonged
bradycardia and inadequate cardiac
output.
Falls and injuries due to syncope.
Reduced quality of life due to chronic
fatigue and other symptoms.
Complications