Downloaded 3,619 times
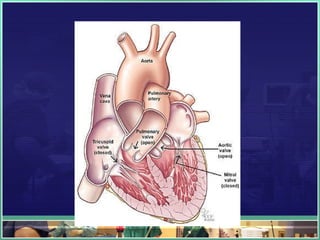
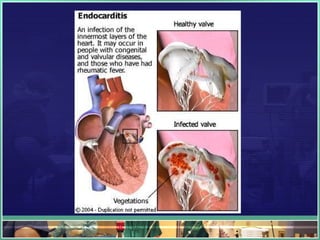
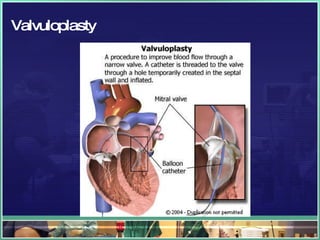
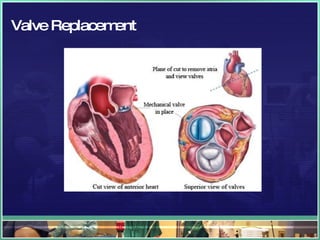
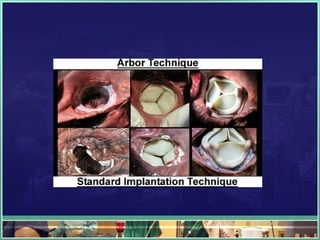
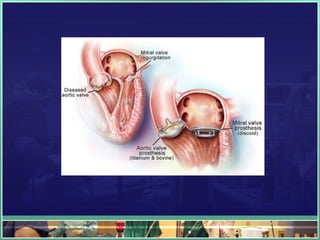

Rheumatic heart disease is a systemic inflammatory disease that commonly affects children between 5-15 years old after a streptococcal throat infection. It involves inflammation of the heart valves and tissue, which can lead to valve damage over time from conditions like endocarditis. Common signs and symptoms include polyarthritis, rash, subcutaneous nodules, and heart murmurs. Diagnosis involves blood tests showing elevated inflammatory markers and echocardiography to evaluate the heart valves and function. Treatment depends on the severity of valve involvement but may include surgery such as valve repair or replacement for severe cases.























































































