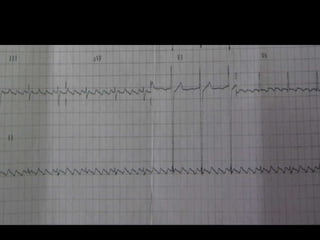
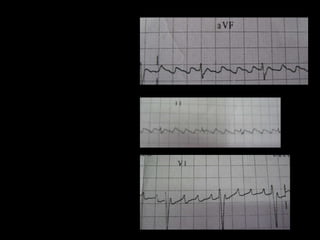
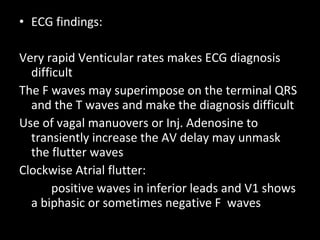
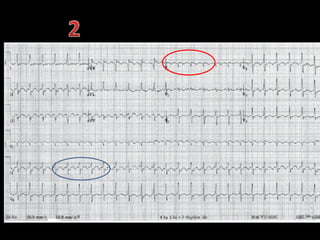
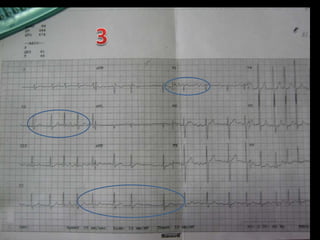
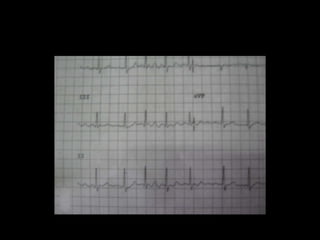
Daniel, a 50-year-old male, presented with palpitations and chest pain for 2 hours. His ECG showed atrial flutter with an atrial rate of 300 beats/min and a 4:1 heart rate of 75 beats/min, indicating incomplete right bundle branch block. Atrial flutter is a macro-reentrant arrhythmia involving a reentrant pathway, most commonly in the cavo-tricuspid isthmus. ECG findings include sawtooth-shaped flutter waves and a constant atrial rate of around 300 beats/min. Treatment involves cardioversion, anticoagulation, antiarrhythmic drugs, or catheter ablation of the reentrant pathway.



































































![ECG [Compatibility Mode].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/ecgcompatibilitymode-230828072404-d338c45c-thumbnail.jpg?width=640&height=640&fit=bounds)








































