Downloaded 222 times

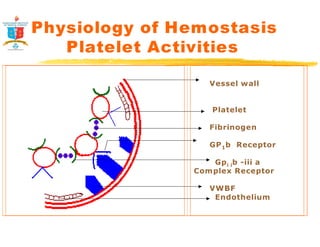
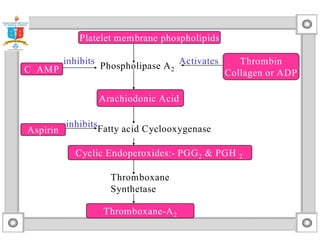
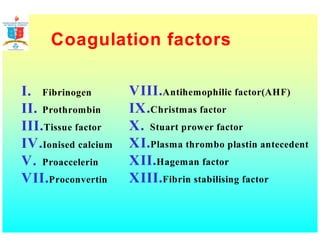
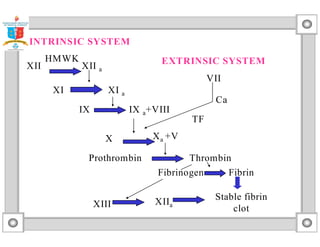
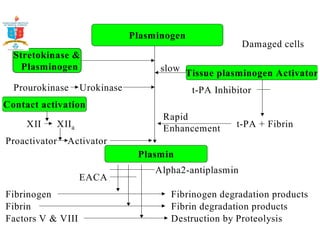
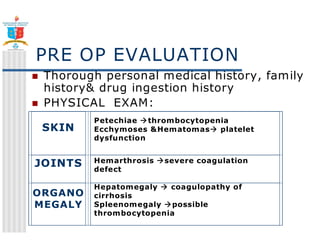
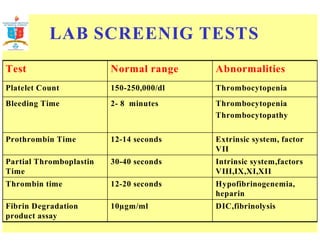
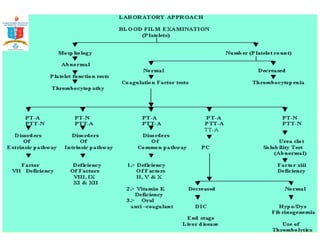
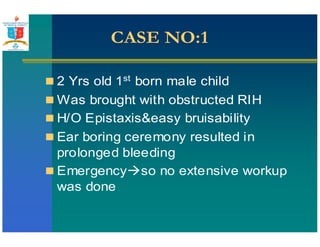
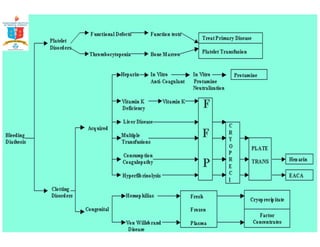
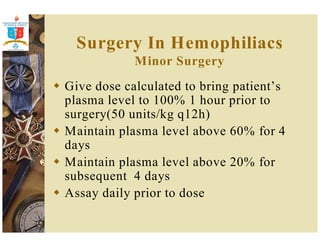
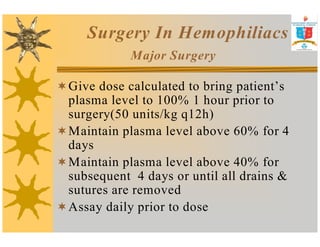
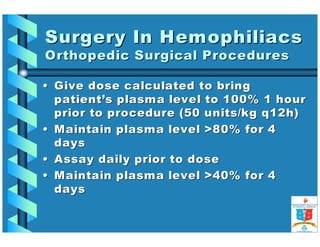


Surgery in patients with bleeding disorders requires careful evaluation and management to minimize bleeding risks. The document discusses: 1) The physiology of hemostasis including the vessel wall, platelet, and coagulation responses. 2) Evaluation of patients including history, exam, and screening tests to identify bleeding disorders. 3) Four case examples of patients who bled excessively during or after surgery, who were found to have thrombocytopathy, hemophilia, or other disorders. 4) Common bleeding disorders surgeons may encounter including thrombocytopenia, thrombocytopathy, hemophilia A/B, von Willebrand disease, DIC, and liver disease. 5) Guidelines

![Angiodysplasia[1]](https://cdn.slidesharecdn.com/ss_thumbnails/angiodysplasia1-190610163612-thumbnail.jpg?width=640&height=640&fit=bounds)


































































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)




