Downloaded 323 times
















































The document summarizes key aspects of haemostasis including the vascular, platelet and coagulation phases. It describes tests used to diagnose bleeding disorders affecting platelets or coagulation factors. Managing dental procedures in patients with bleeding disorders requires modifying treatment based on the nature and severity of the disorder to minimize risks of bleeding. Pre-operative assessment of bleeding history and factors is important to guide management and prevent post-operative bleeding complications.
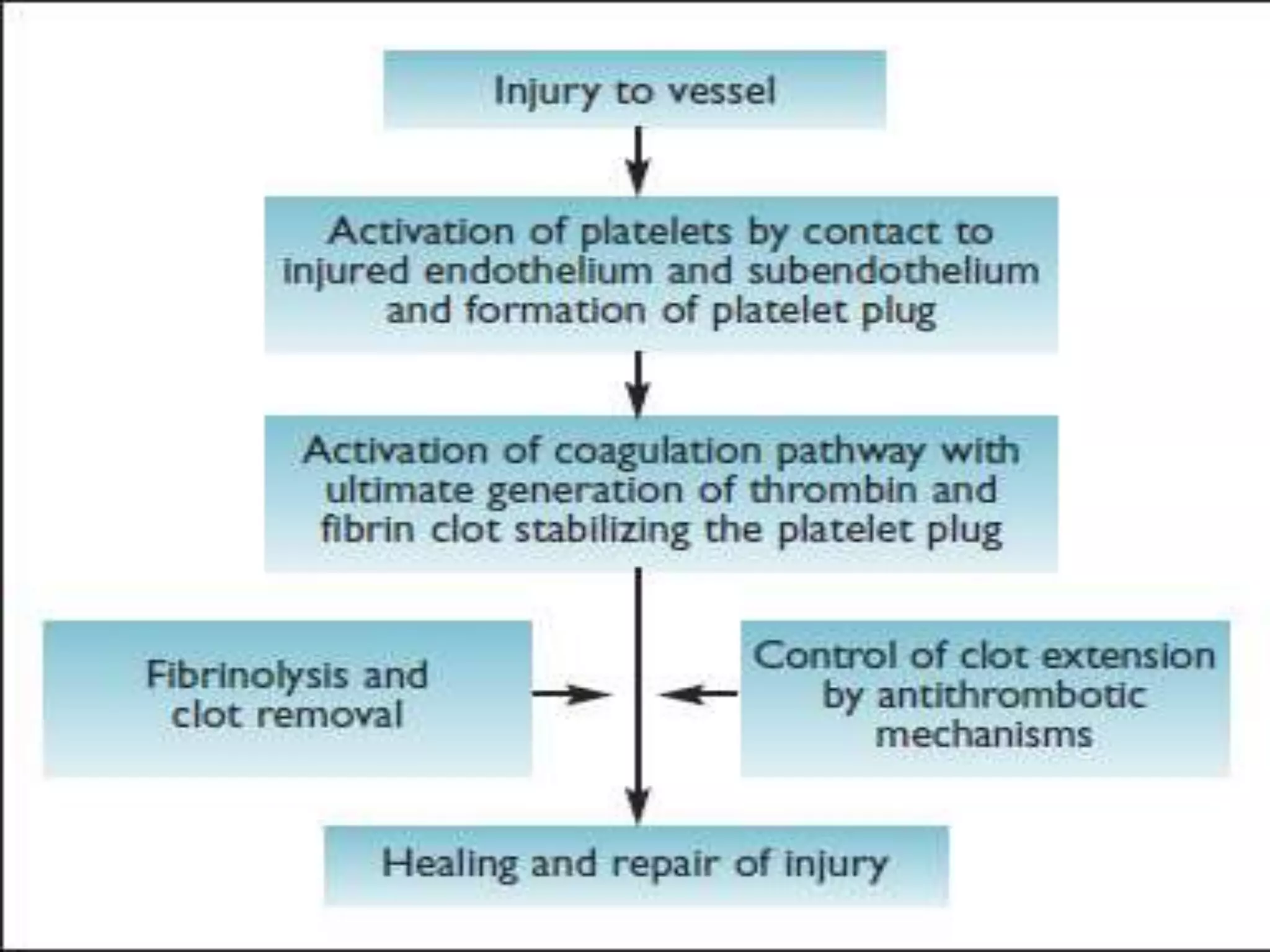
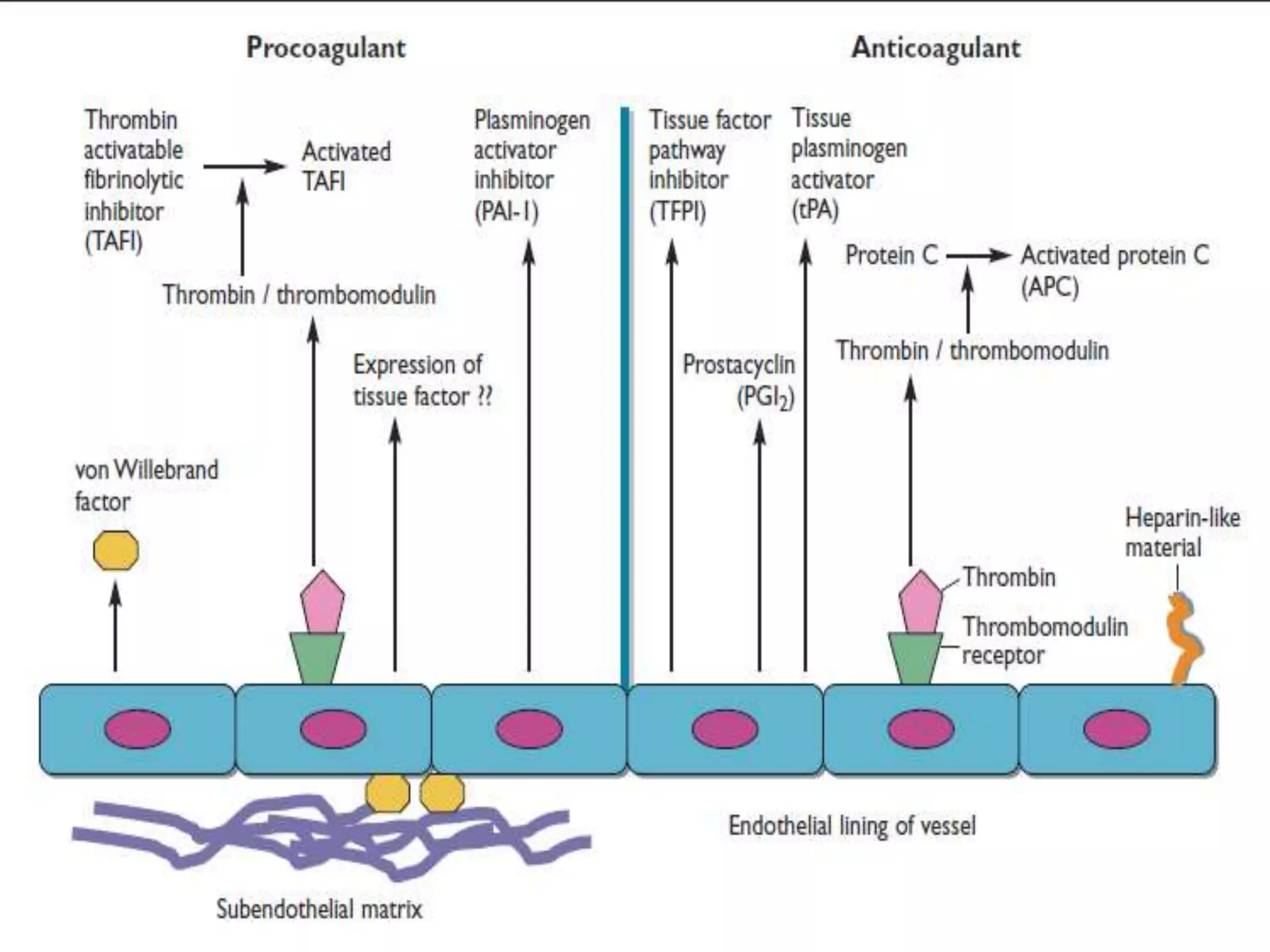
Introduction to haemostasis, its phases like vascular and platelet phase, and its role in preventing bleeding.
Breakdown of haemostasis stages focusing on the vascular and platelet phases essential for clot formation.
Breakdown of haemostasis stages focusing on the vascular and platelet phases essential for clot formation.
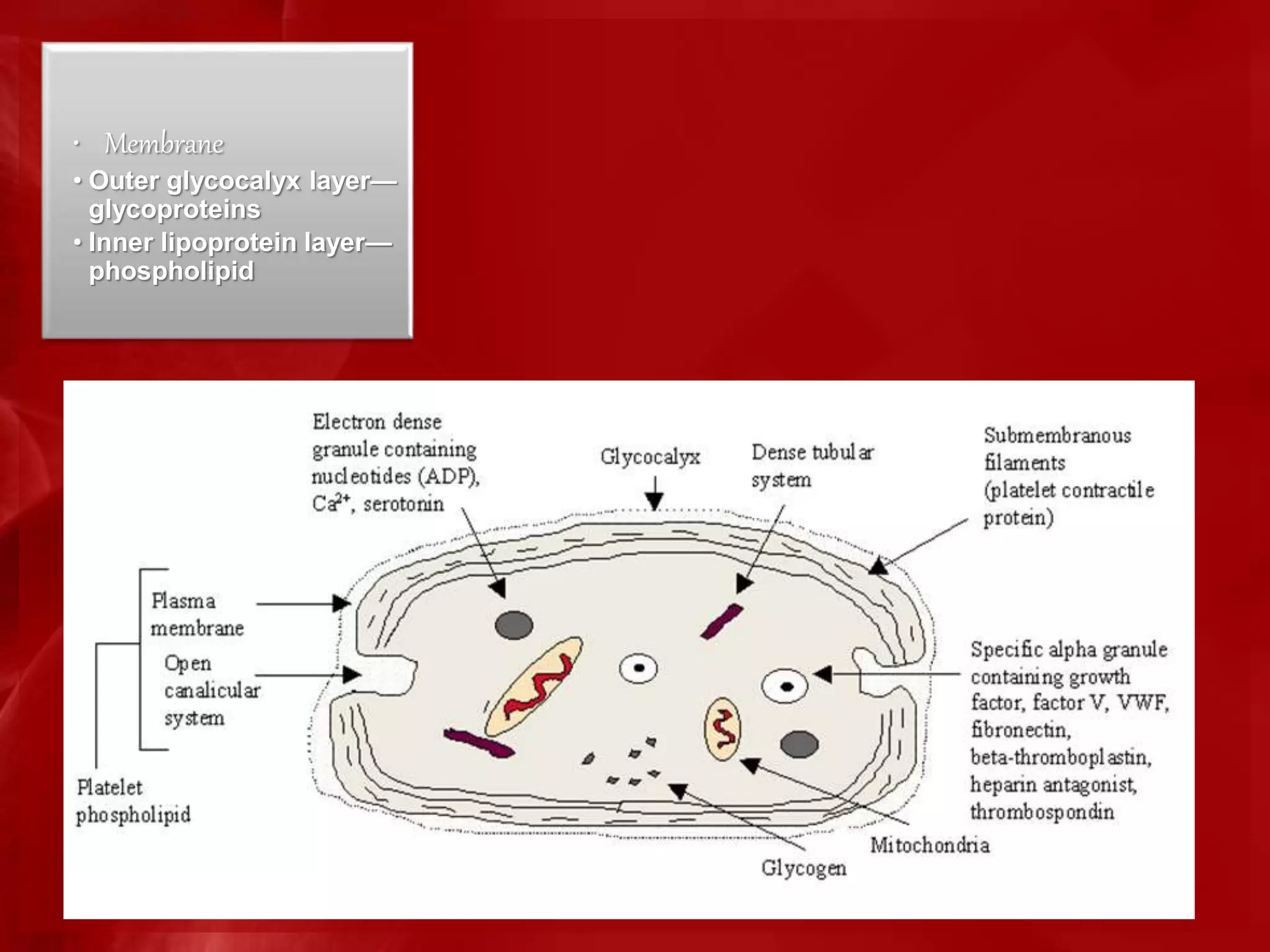
Platelet count (150,000-400,000 per cu mm) and lifespan (9-12 days), including structure and role in clot formation.
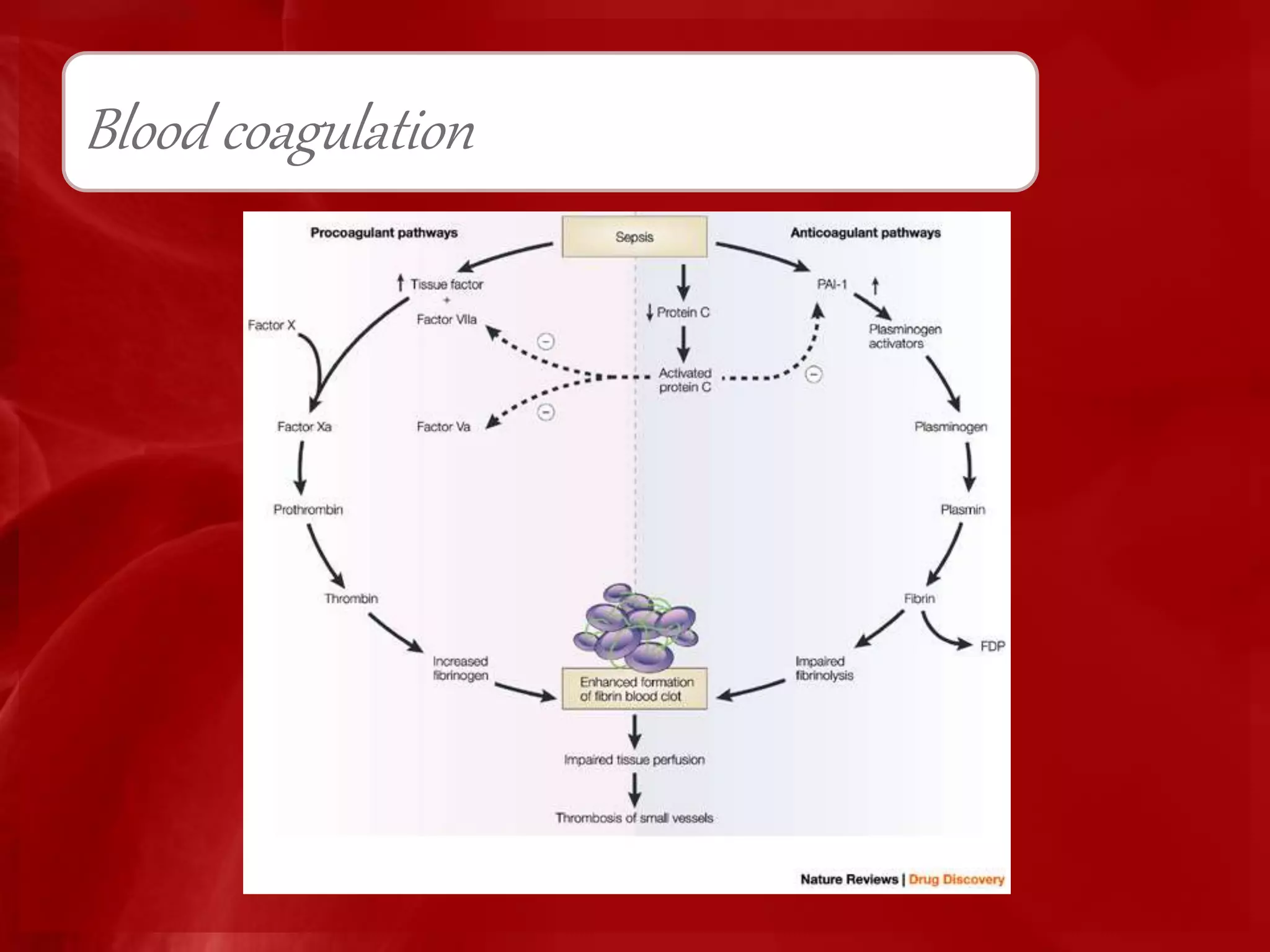
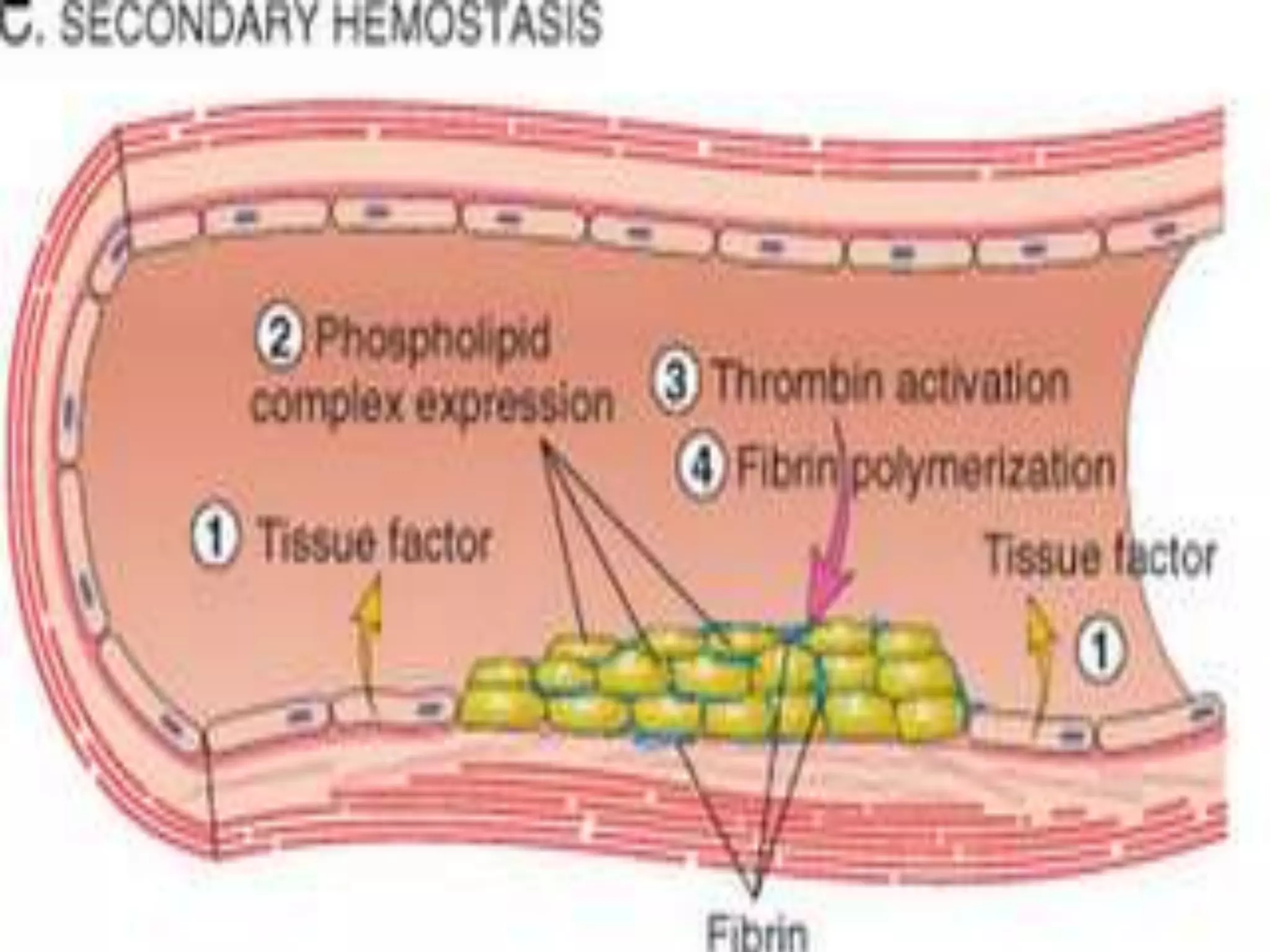
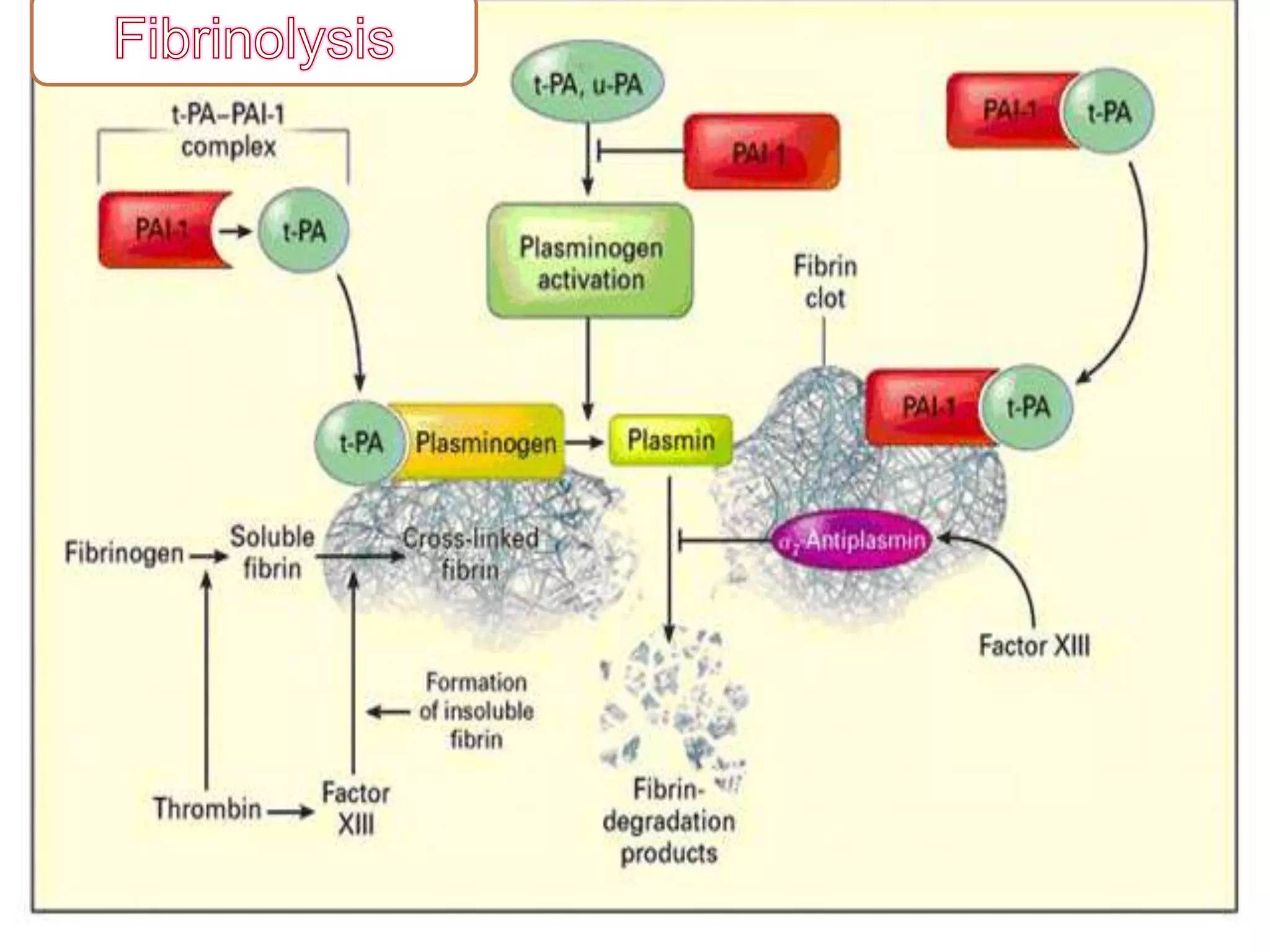
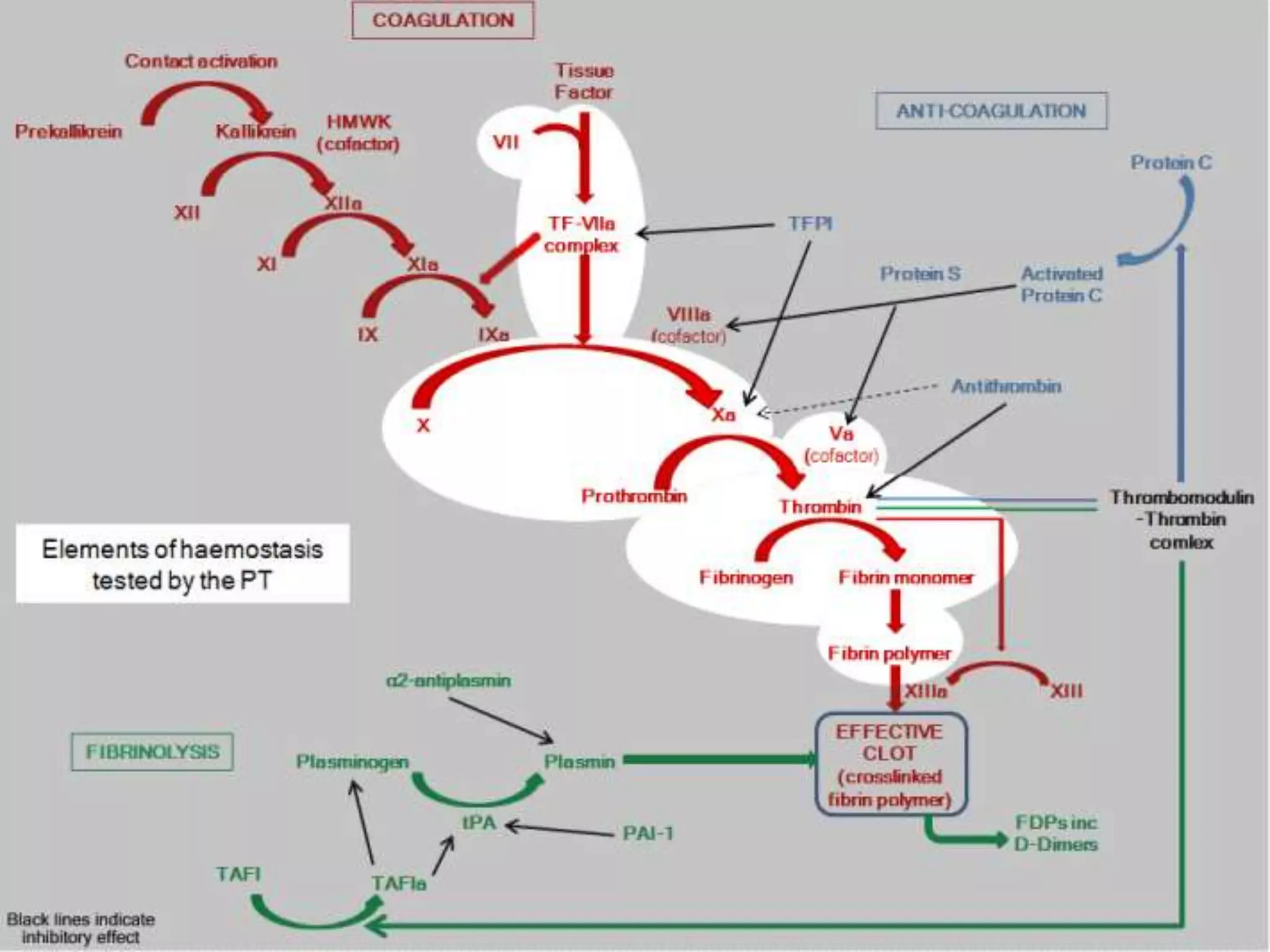
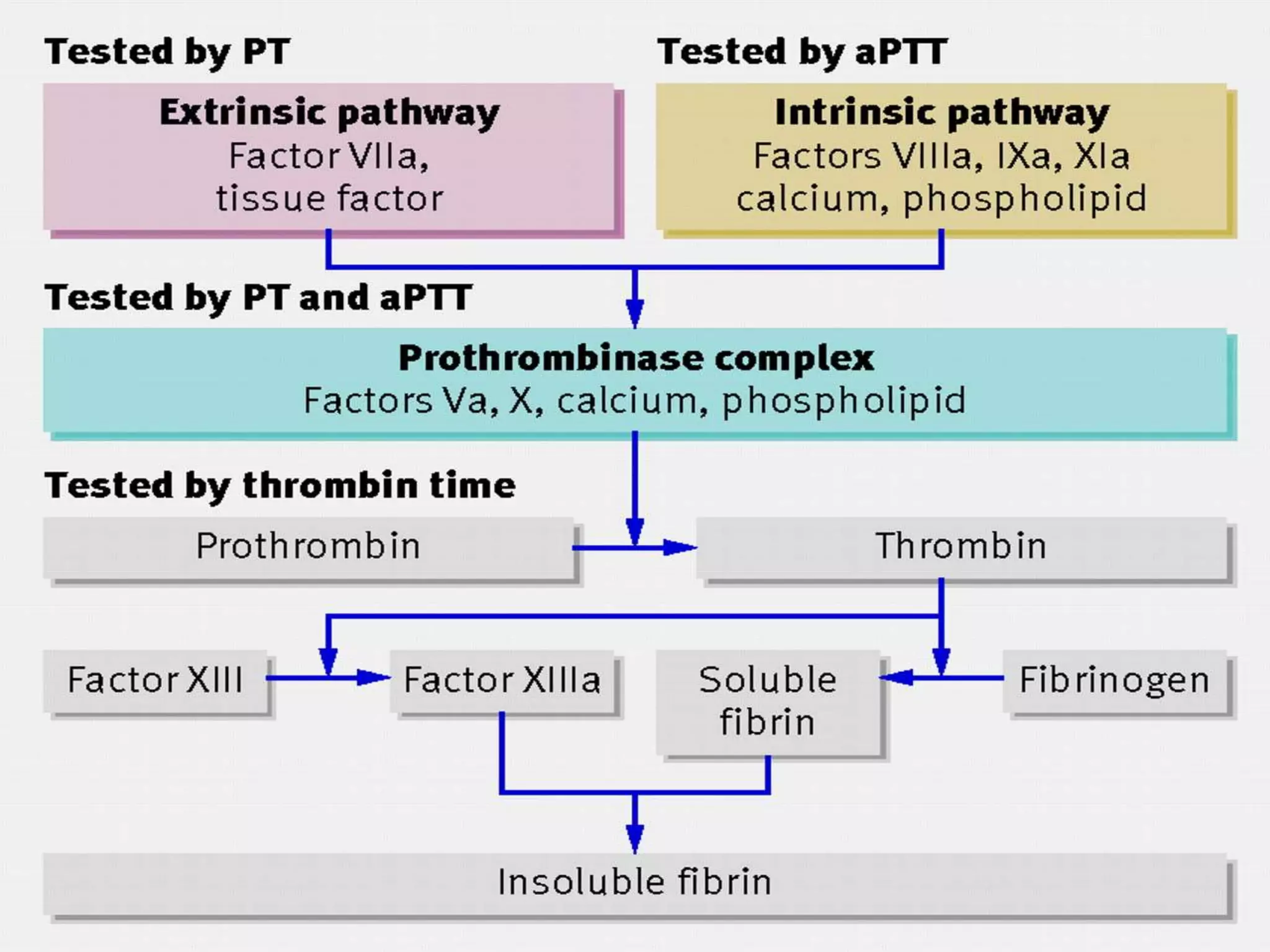
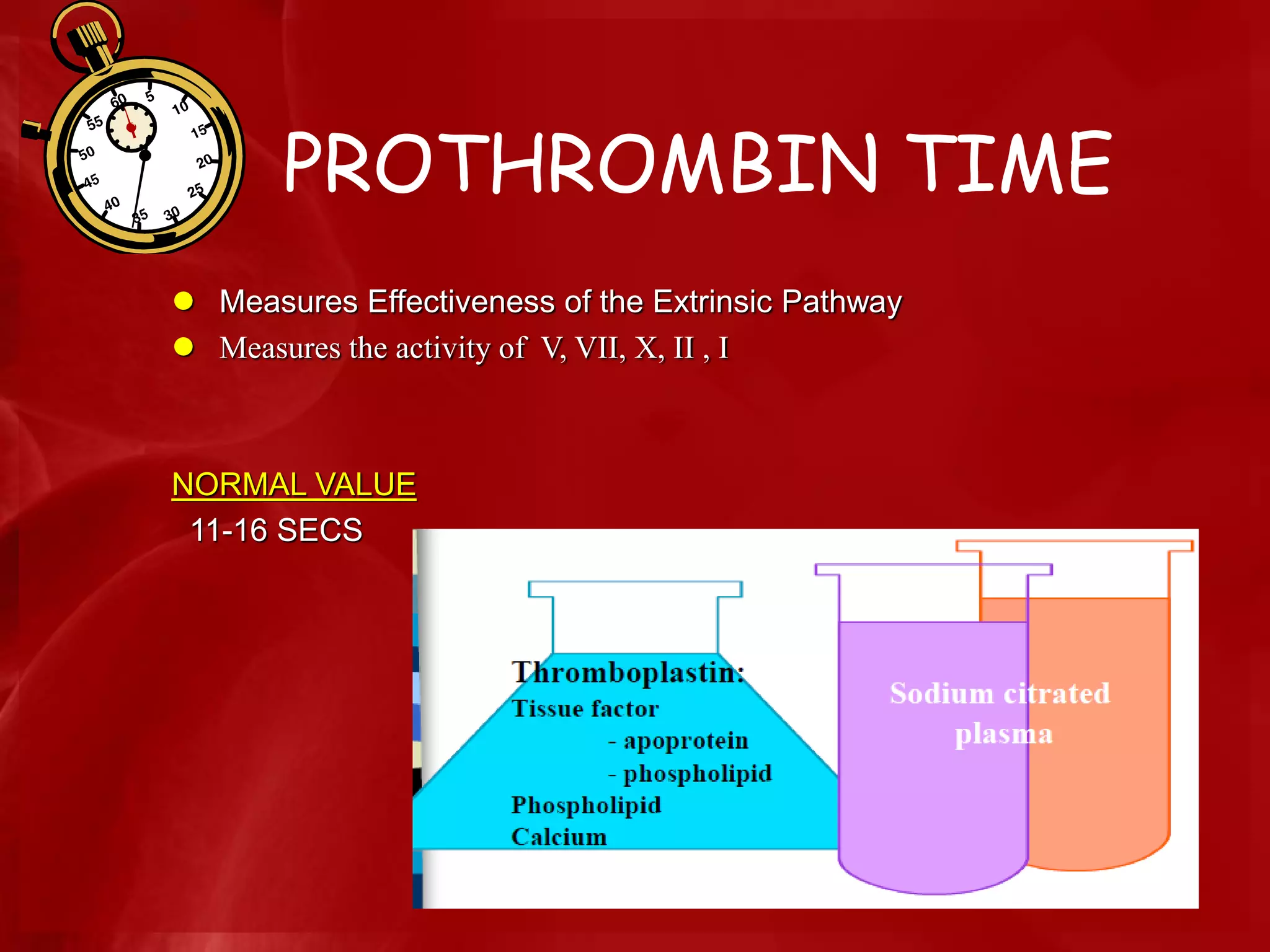
Details of blood coagulation involving thrombin action, fibrin formation and the structural aspects of clot.
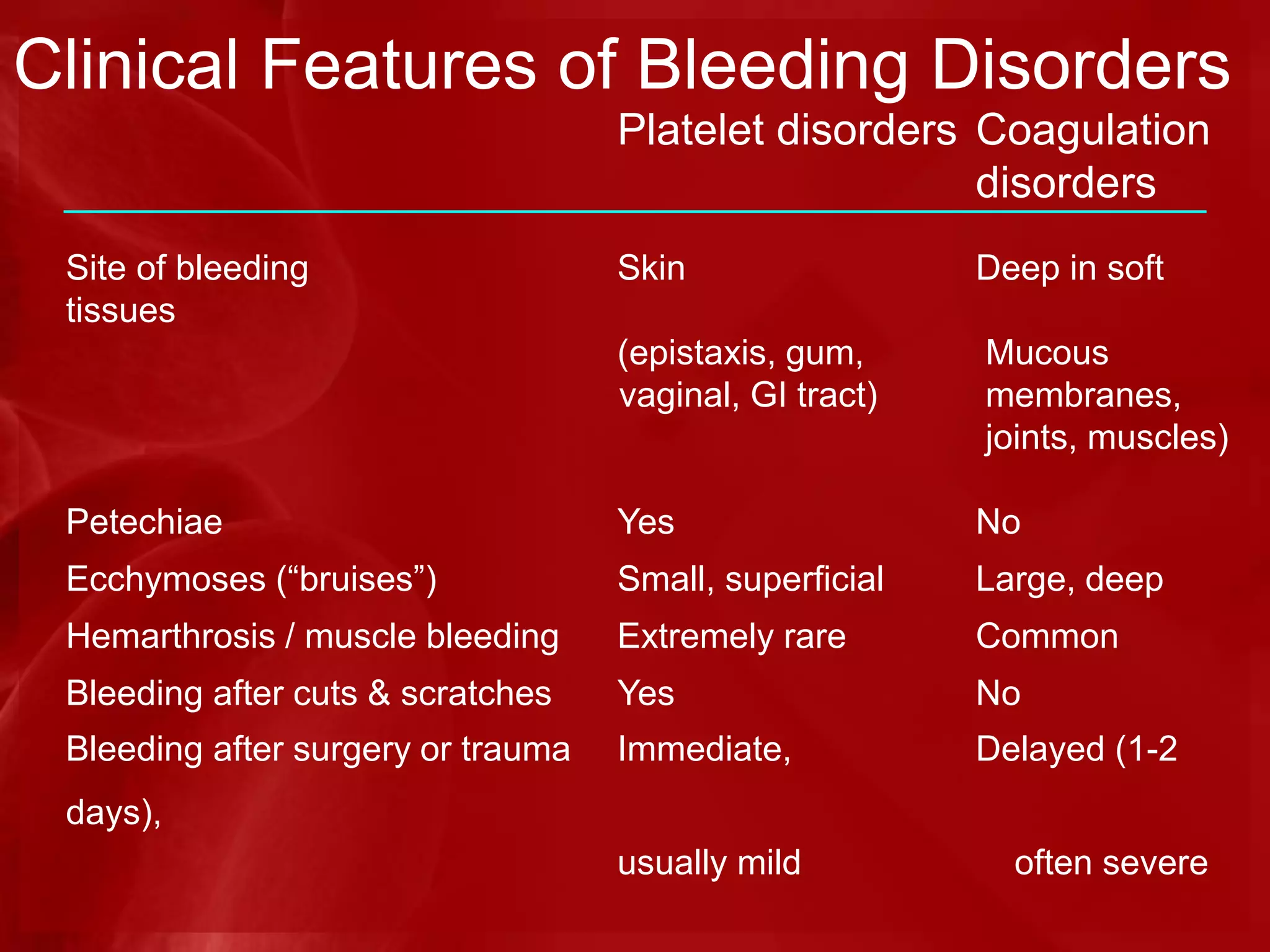
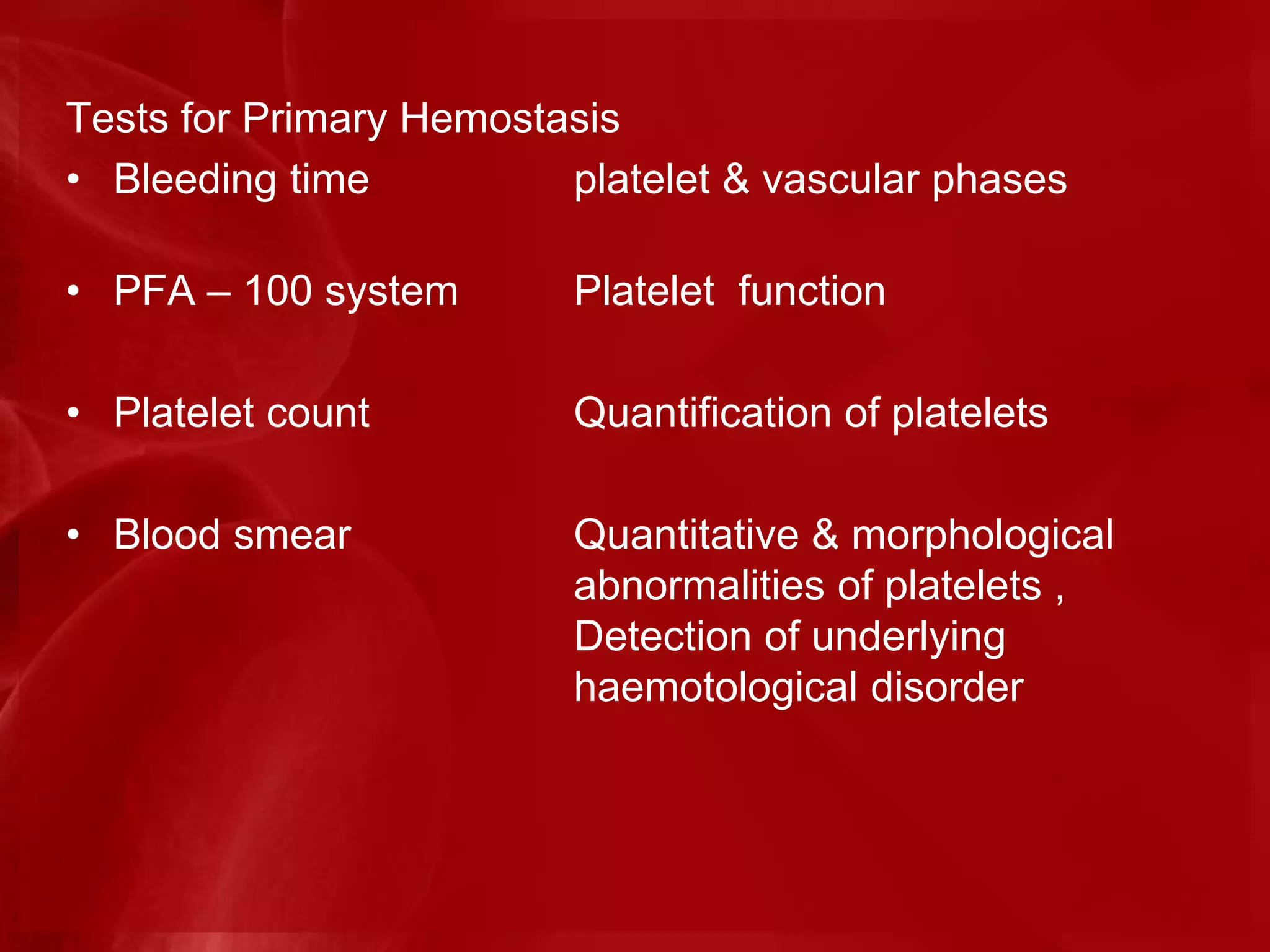
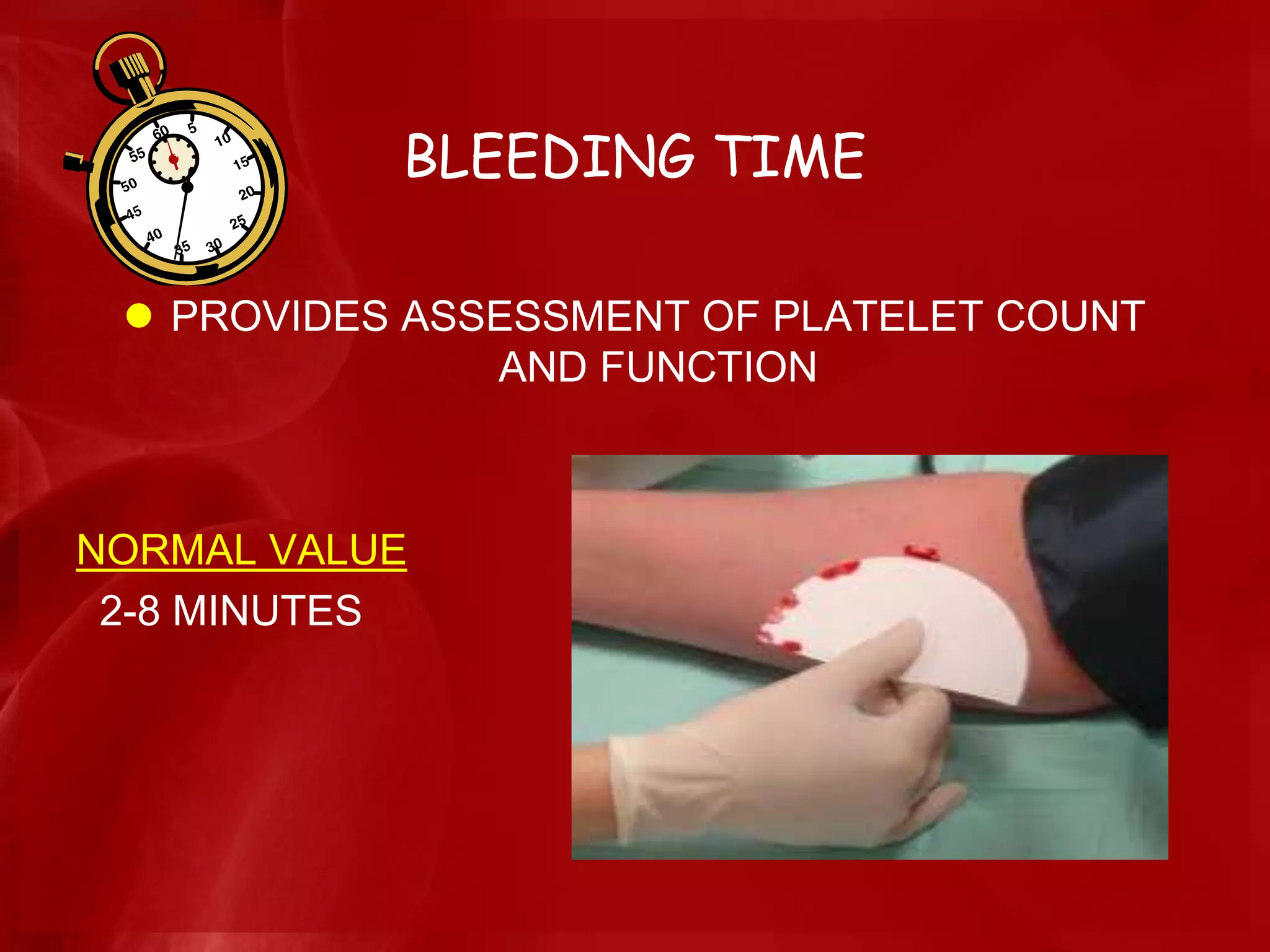
Approach to diagnosing bleeding disorders, including clinical and laboratory evaluations for inherited/acquired causes.Differentiation between inherited and acquired bleeding disorders, detailing types like vasculopathies and coagulopathies.
Pre-operative management and treatment modifications based on patient history, including medication considerations and surgical precautions.
Acknowledgment of sources used for the presentation materials and concluding thoughts.


































![Hematology%20disorder%20in%20dental%20treatment[1]](https://cdn.slidesharecdn.com/ss_thumbnails/hematology20disorder20in20dental20treatment1-161105033248-thumbnail.jpg?width=640&height=640&fit=bounds)




















































