Downloaded 170 times
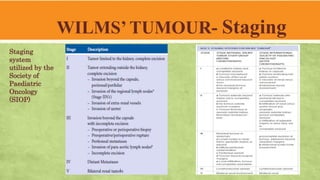
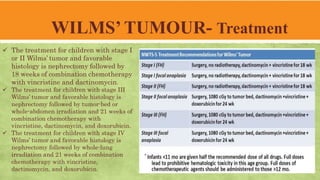


Wilms' tumor, or nephroblastoma, is the most common renal tumor in children aged 2 to 4, typically presenting as an asymptomatic abdominal mass. The overall survival rate is 85% due to advancements in diagnosis and treatment, with approaches varying between different organizations like the Children Oncology Group and the International Society of Pediatric Oncology. Diagnosis and staging involve various imaging techniques, and treatment typically includes nephrectomy followed by chemotherapy and/or radiotherapy, depending on the disease stage and histology.






























![Wilm's tumour - The most common kidney tumor in children - Dr Vishnu A [VCR],...](https://cdn.slidesharecdn.com/ss_thumbnails/vishnu-wilmstumour-210312145616-thumbnail.jpg?width=640&height=640&fit=bounds)












































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)










