Contents (Based on PBNS and BSN curriculum of PU)
- Common terminologies
- Characteristics of aging
- Normal aging process
- Concept of healthy aging
- Need of elderly people (Health promotion and Maintenance of Elderly people
- Developmental tasks of elderly people
- Theory of Aging
* Biological theory
* Psychological theory
* Sociological theory
* Environmental theory
* Developmental theory
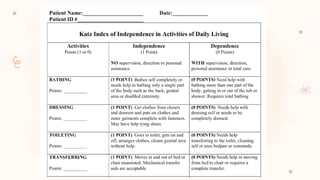
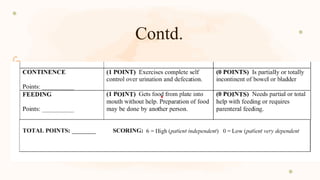
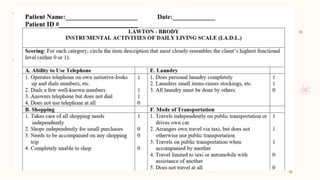
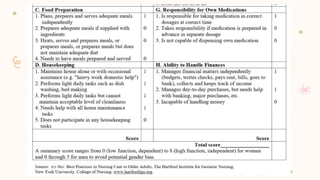
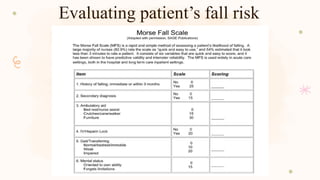
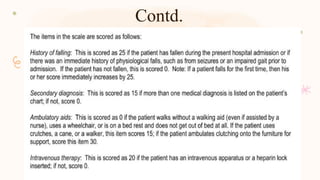
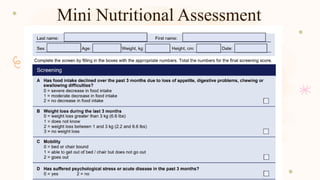
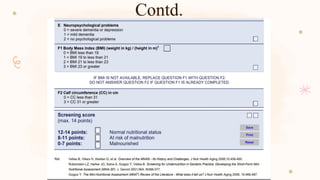
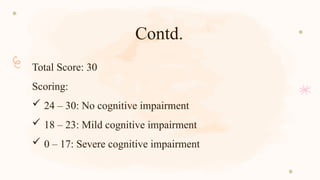
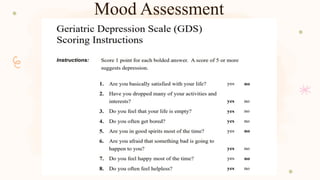
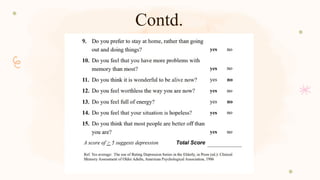
- Geriatric Assessment
- Contributions of the elderly to the young generation
- Nurses' roles and responsibilities for elderly
- Self care Model in Gerontology

































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)






![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




