Downloaded 2,155 times



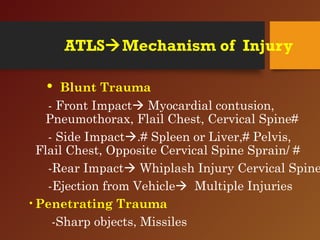
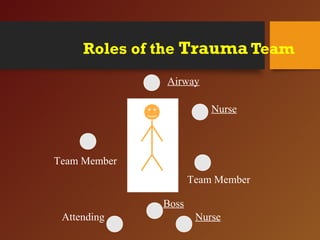
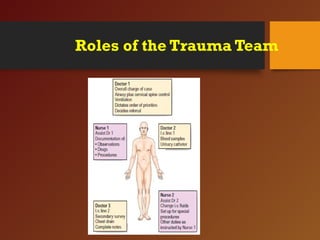
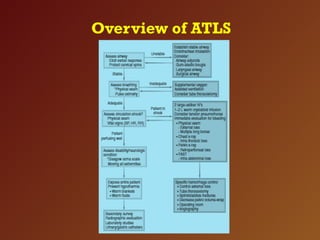


The document provides an overview of Advanced Trauma Life Support (ATLS) principles and practices, outlining the objectives, phases of trauma management, and critical assessments for trauma patients. It emphasizes the importance of rapid assessment, early intervention, and organized care in critical situations, detailing the primary and secondary survey components, triage processes, and resuscitation techniques. Key points include the recognition of life-threatening conditions and the roles of multidisciplinary trauma teams in managing patients effectively.













































![Advanced Trauma Life Support [ATLS] and Triage](https://cdn.slidesharecdn.com/ss_thumbnails/atlstriage-251212075759-fbe88f4f-thumbnail.jpg?width=640&height=640&fit=bounds)





























![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)








