Download as PDF, PPTX


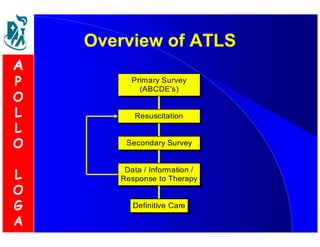
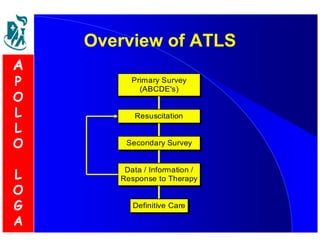

Advanced Trauma Life Support (ATLS) is a system to rapidly assess and treat trauma patients. It focuses on the initial care of trauma patients, with an emphasis on the first hour known as the "golden hour." The goal of ATLS is to rapidly identify and intervene in life-threatening injuries through a primary and secondary survey, resuscitation, and stabilization of the patient for transfer to the operating room or intensive care unit if needed. ATLS aims to minimize mortality and morbidity through structured training programs for medical professionals in trauma care.

























































![Advanced Trauma Life Support [ATLS] and Triage](https://cdn.slidesharecdn.com/ss_thumbnails/atlstriage-251212075759-fbe88f4f-thumbnail.jpg?width=640&height=640&fit=bounds)



































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)











