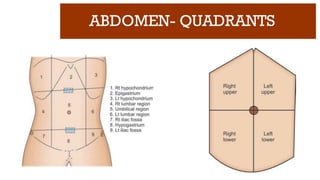
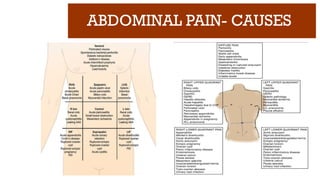
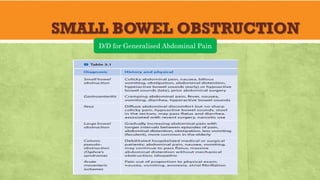
ABDOMINAL PAIN- CAUSES
✓Inflammation of a viscus
✓ Perforation of a viscus
✓ Obstruction of a viscus
✓ Infarction of a viscus
✓ Intra-abdominal hemorrhage or retroperitoneal hemorrhage
✓ Extra-abdominal or medical causes for acute abdominal pain like lower lobe
pneumonia and inferior wall MI
6.
ABDOMINAL PAIN- HISTORY
SOCRATES= Nemonic
S - site
O - onset
C - characteristics
R - radiation
A – associated symptoms &
signs
T - timing
E - exacerbating/
alleviating
S - severity
✓ “S” stands for “site”. Which region/quadrant? Is
it a general sense of overall discomfort? The site
of pain helps you fine tune your subsequent
physical exam and diagnostic decision making.
✓ “O” stands for “onset”. When did the pain start?
Acute or insidious?
✓ “C” stands for “characteristics”. The pain may
be sharp, dull, heavy, etc. or a combination of
descriptions.
7.
ABDOMINAL PAIN- HISTORY
SOCRATES= Nemonic
S - site
O - onset
C - characteristics
R - radiation
A – associated symptoms &
signs
T - timing
E - exacerbating/
alleviating
S - severity
✓ “R”, which represents “radiation”. Ask if the
pain stays at the site they are describing or if it
travels somewhere else in the body. Ex:Ureteric
colic
✓ A” stands for associated symptoms. What other
symptoms are present and associated with the
pain? Ask do they also have nausea and/or
vomiting?
✓ "T" stands for timing. When does the pain
occur? Does it happen at specific times of the
day, or is it constant?
8.
ABDOMINAL PAIN- HISTORY
SOCRATES= Nemonic
S - site
O - onset
C - characteristics
R - radiation
A – associated symptoms &
signs
T - timing
E - exacerbating/
alleviating
S - severity
✓ “E” represents “exacerbating” factors; grouped
within this is also alleviating factors. The
patient should be probed as to what makes their
pain better or worse. Certain physical positions,
medications, etc. These factors can all provide
historical clues about the root cause.
✓ “S” stands for “severity”. In most hospitals this
is formulated on a 1 to 10 scale with 10 being
the most severe pain they’ve ever experienced.
9.
ABDOMINAL PAIN
✓Somatic pain:
✓Originatefrom abdominal wall
and parietal peritoneum
✓Sharper and more distinct
✓Better localized
✓Sensitive to cutting,tearing,
burning and crushing
✓Visceral pain:
✓Originate from internal organs
and visceral peritoneum
✓Achy and crampy
✓Variable localization and
sensation
✓Not sensitive to cutting, tearing,
burning or crushing
✓Sensitive to stretching of walls of
hollow organs and capsule of
solid organs
10.
ABDOMINAL PAIN
✓Shifting pain:Ex: Periumbilical pain shifting to RLQ in
Ac.appendicitis
✓Radiating pain: Ex: Pain radiating from loin to groin in ureteric
colic
✓Reffered pain: Ex: Pain felt at Lt shoulder in case of splenic
rupture
11.
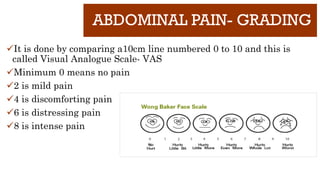
ABDOMINAL PAIN- GRADING
✓Itis done by comparing a10cm line numbered 0 to 10 and this is
called Visual Analogue Scale- VAS
✓Minimum 0 means no pain
✓2 is mild pain
✓4 is discomforting pain
✓6 is distressing pain
✓8 is intense pain
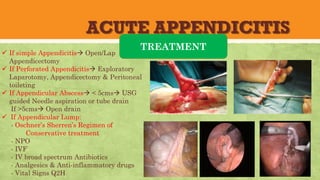
ACUTE APPENDICITIS
Objectives
ü Causesof RLQ Pain
ü Etiology
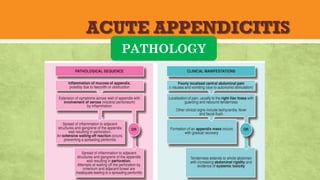
ü Pathology
ü Clinical features- Symptoms & Signs
ü Investigations
ü Scoring System
ü Treatment
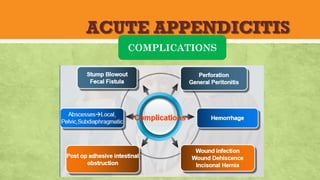
ü Complications
ü Mindmap
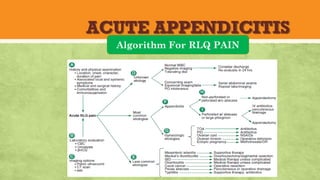
ü Algorithm for RLQ Pain
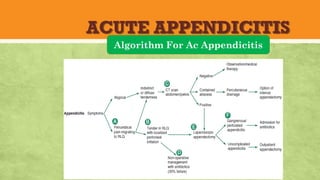
ü Treatment Algorithm for Ac Appendicitis
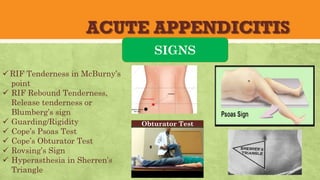
ACUTE APPENDICITIS
SIGNS
üRIF Tendernessin McBurny’s
point
ü RIF Rebound Tenderness,
Release tenderness or
Blumberg’s sign
ü Guarding/Rigidity
ü Cope’s Psoas Test
ü Cope’s Obturator Test
ü Rovsing’s Sign
ü Hyperasthesia in Sherren’s
Triangle
Obturator Test
20.
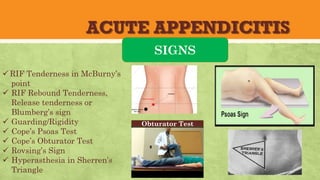
ACUTE APPENDICITIS
SIGNS
üRIF Tendernessin McBurny’s
point
ü RIF Rebound Tenderness,
Release tenderness or
Blumberg’s sign
ü Guarding/Rigidity
ü Cope’s Psoas Test
ü Cope’s Obturator Test
ü Rovsing’s Sign
ü Hyperasthesia in Sherren’s
Triangle
Obturator Test
21.
ACUTE APPENDICITIS
INVESTIGATIONS
üLab investigations:
1.Total WBC and Differential counts
2. C-Reactive Protein- CRP
2. Urine- FEME if positive for C&S
3. B- HCG to R/O pregnancy
ü Imaging studies:
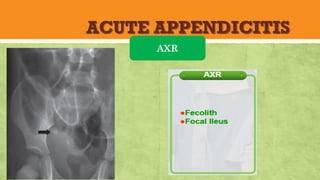
1. CXR- Erect or AXR including both side diaphragm to R/O Pneumoperitoneum
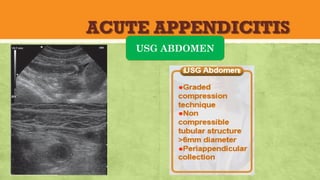
2. USG-To R/O any other pathology in women of child bearing age group
3. USG-To confirm Appendicitis
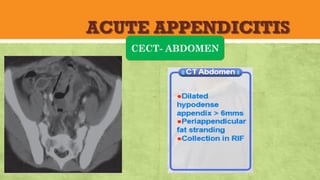
4. CECT abdomen
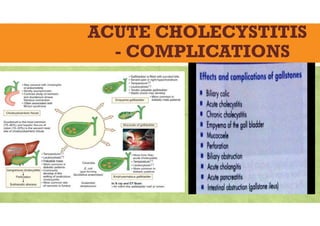
ACUTE CHOLECYSTITIS
-Epidemiology
Cholecystitisis inflammation of the
gallbladder most commonly due to an
obstruction of the cystic duct by gallstones
arising from the gallbladder (cholelithiasis).
Uncomplicated cholecystitis has an excellent
prognosis; the development of complications
such as perforation or gangrene renders a bad
prognosis.
10%-20% of Americans have gallstones, and as
many as one third of these people develop
acute cholecystitis
AGE: The incidence of cholecystitis increases
with age. Explanation for this is unclear.
Sex distribution: Gallstones are 2-3 times
more frequent in females than in males,
resulting in a higher incidence of calculous
cholecystitis in females. Elevated progesterone
levels during pregnancy is the cause.
Acalculous cholecystitis is observed more often
in elderly men.
Prevalence by race and ethinicity: More
common in people of Scandinavian descent,
Pima Indians, and Hispanic populations. In
the United States, white people have a higher
prevalence than black people.
37.
ACUTE CHOLECYSTITIS
-ETIOLOGY
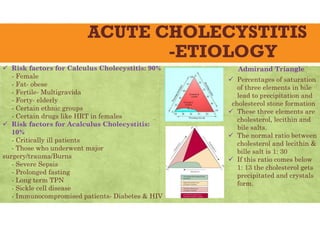
Riskfactors for Calculus Cholecystitis: 90%
- Female
- Fat- obese
- Fertile- Multigravida
- Forty- elderly
- Certain ethnic groups
- Certain drugs like HRT in females
Risk factors for Acalculus Cholecystitis:
10%
- Critically ill patients
- Those who underwent major
surgery/trauma/Burns
- Severe Sepsis
- Prolonged fasting
- Long term TPN
- Sickle cell disease
- Immunocompromised patients- Diabetes & HIV
Admirand Triangle
Percentages of saturation
of three elements in bile
lead to precipitation and
cholesterol stone formation
These three elements are
cholesterol, lecithin and
bile salts.
The normal ratio between
cholesterol and lecithin &
bille salt is 1: 30
If this ratio comes below
1: 13 the cholesterol gets
precipitated and crystals
form.
38.
ACUTE CHOLECYSTITIS
-PATHOLOGY
90%of cases of cholecystitis involve
calculous cholecystitis, with the other
10% of cases representing acalculous
cholecystitis.
Acute calculous cholecystitis is caused
by an obstruction of the cystic duct,
leading to distention of the gallbladder.
As the gallbladder becomes distended,
blood flow and lymphatic drainage are
compromised, leading to mucosal
ischemia and necrosis.
Acalculous cholecystitis- exact
mechanism is unclear. Injury may be
the result of retained concentrated bile.
Stage 1: stone lodges in cystic
duct; midepigastric colickypain
Stage 2: stone impacts in cystic
duct; pain shift to RUQ;
radiation to right
scapula/shoulder
Stage 3: bacterial invasion GB
wall; + Murphy sign; subsides if
stone falls out
Stage 4: perforation
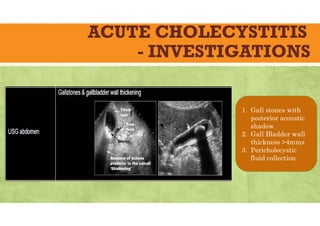
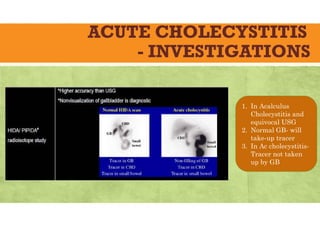
ACUTE CHOLECYSTITIS
- INVESTIGATIONS
1.In Acalculus
Cholecystitis and
equivocal USG
2. Normal GB- will
take-up tracer
3. In Ac cholecystitis-
Tracer not taken
up by GB
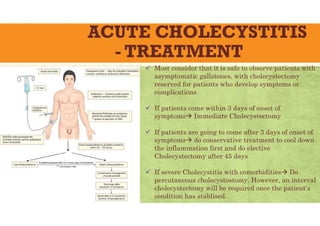
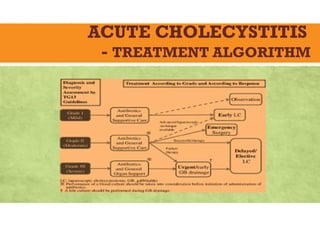
ACUTE CHOLECYSTITIS
- TREATMENT
Most consider that it is safe to observe patients with
asymptomatic gallstones, with cholecystectomy
reserved for patients who develop symptoms or
complications
If patients come within 3 days of onset of
symptoms Immediate Cholecystectomy
If patients are going to come after 3 days of onset of
symptoms do conservative treatment to cool down
the inflammation first and do elective
Cholecystectomy after 45 days
If severe Cholecystitis with comorbidities Do
percutaneous cholecystostomy. However, an interval
cholecystectomy will be required once the patient’s
condition has stablised.
ACUTE PANCREATITIS
ü Differentcauses for epigastric pain
ü Epidemiology
ü Classifications and definitions
ü Etiology
ü Pathology
ü Clinical features
ü Investigations
ü Assessment of severity
ü Treatment
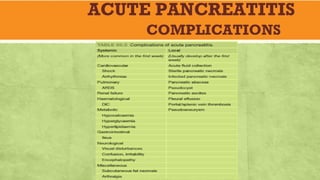
ü Complications
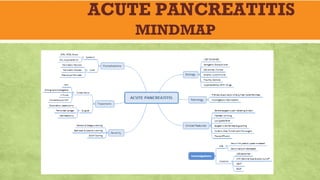
ü Mindmap
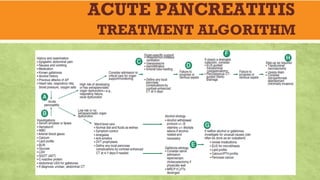
ü Treatment Algorithm
ACUTE PANCREATITIS
-Epidemiology
ü Pancreatitisis inflammation of the pancreas .
It is one of the most devastating conditions in
the abdomen.
ü More than 75% of cases of acute pancreatitis
are due to either gallstones or alcohol.
ü 80% to 85% of patients have mild and self-
limiting Pancreatitis, while 15% to 20% of
patients have severe Acute Pancreatitis
complicated by shock, sepsis, and MODS.
ü The overall mortality for AP is approximately
10% , but in its most severe form , it can
increase to 20% to 30 % .
ü The disease may occur at any age, with a
peak in young men and older women.
ü In the United States, more than 200,000
patients are hospitalized annually with acute
pancreatitis
ü It is the principal cause of approximately
3,200 deaths per year
ü Infection of pancreatic and peripancreatic
necrosis complicates 30% to 70% of cases of
acute necrotizing pancreatitis and occurs
during the second to third weeks after onset
of disease.
54.
ACUTE PANCREATITIS
CLASSIFICATIONS ANDDEFINITIONS
Atlanta classification of acute pancreatitis(1992)
ü Mild acute pancreatitis:
● no organ failure;
● no local or systemic complications.
ü Moderately severe acute pancreatitis:
● organ failure that resolves within 48 hours
(transient organ failure); and/or
● local or systemic complications without
persistent organ failure.
ü Severe acute pancreatitis:
● persistent organ failure (>48 hours);
● single organ failure
● multiple organ failure.
55.
ACUTE PANCREATITIS
-ETIOLOGY
Nemonic: “IGET SMASHED”:
ü Idiopathic
ü Gallstones
ü Ethanol
ü Trauma
ü Scorpion bite
ü Mumps (viruses)
ü Autoimmune
ü Steroids
ü Hyperlipidemia
ü ERCP
ü Drugs like Azathioprine,Thiazide.Valproic acid
and Sulfasalazine.
ACUTE PANCREATITIS
-Clinical Features
üSevere epigastric pain radiating
straight to the back
ü This pain is relieved on bending
forwards
ü Anorexia, nausea and vomiting
ü Low grade fever
üMid-epigastric tenderness &
fullness (paralytic ileus)
üCullen’s sign ( peri-umbilical
discoloration)
üGrey Turner’s sign (discoloration
of flanks)
üFox’s sign ( discoloration around
inguinal ligament)
üEpigastric guarding
üPleural effusion
SYMPTOMS SIGNS
58.
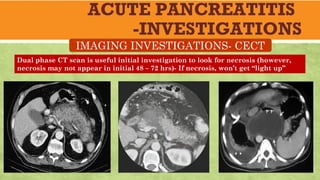
ACUTE PANCREATITIS
-INVESTIGATIONS
ü WBCs:↑
ü Hct: ↑ (in dehydration)/ ↓ (in
hemorrhage)
ü ABG: metabolic & respiratory
acidosis + hypoxia
ü Urinary amylase: ↑
LAB INVESTIGATIONS
Serum
ü Lipase: ↑↑ (more specific &
sensitive)
ü Amylase: ↑↑↑ (less specific)
ü BUN, creatinine: ↑
ü Liver enzymes, bilirubin: ↑
ü Inflammatory markers (CRP,
IL-6, IL-8): ↑
ü Glucose: ↑
ü Ca2+: ↓
ACUTE PANCREATITIS
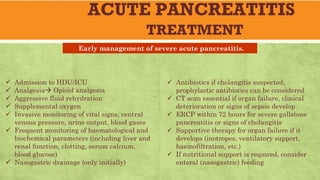
TREATMENT
ü Admissionto HDU/ICU
ü Analgesia Opioid analgesia
ü Aggressive fluid rehydration
ü Supplemental oxygen
ü Invasive monitoring of vital signs, central
venous pressure, urine output, blood gases
ü Frequent monitoring of haematological and
biochemical parameters (including liver and
renal function, clotting, serum calcium,
blood glucose)
ü Nasogastric drainage (only initially)
ü Antibiotics if cholangitis suspected;
prophylactic antibiotics can be considered
ü CT scan essential if organ failure, clinical
deterioration or signs of sepsis develop
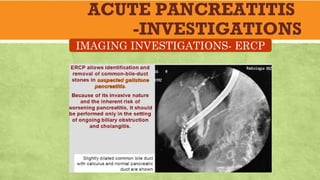
ü ERCP within 72 hours for severe gallstone
pancreatitis or signs of cholangitis
ü Supportive therapy for organ failure if it
develops (inotropes, ventilatory support,
haemofiltration, etc.)
ü If nutritional support is required, consider
enteral (nasogastric) feeding
Early management of severe acute pancreatitis.
68.
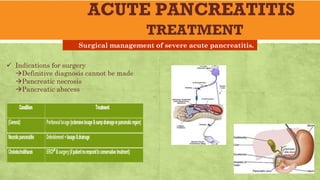
ACUTE PANCREATITIS
TREATMENT
ü Indicationsfor surgery
Definitive diagnosis cannot be made
Pancreatic necrosis
Pancreatic abscess
Surgical management of severe acute pancreatitis.
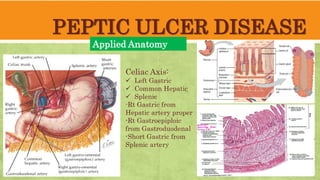
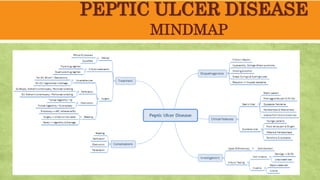
PEPTIC ULCER DISEASE
AppliedAnatomy
Celiac Axis:
Left Gastric
Common Hepatic
Splenic
-Rt Gastric from
Hepatic artery proper
-Rt Gastroepiploic
from Gastroduodenal
-Short Gastric from
Splenic artery
77.
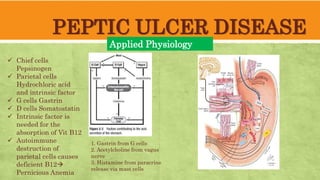
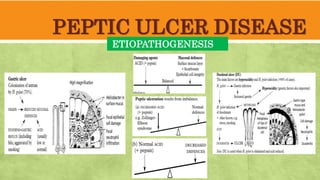
PEPTIC ULCER DISEASE
AppliedPhysiology
Chief cells
Pepsinogen
Parietal cells
Hydrochloric acid
and intrinsic factor
G cells Gastrin
D cells Somatostatin
Intrinsic factor is
needed for the
absorption of Vit B12
Autoimmune
destruction of
parietal cells causes
deficient B12
Pernicious Anemia
1. Gastrin from G cells
2. Acetylcholine from vagus
nerve
3. Histamine from paracrine
release via mast cells
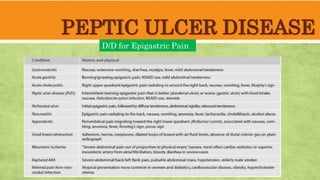
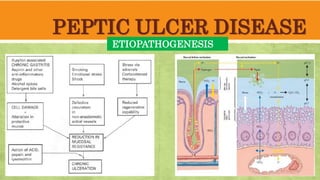
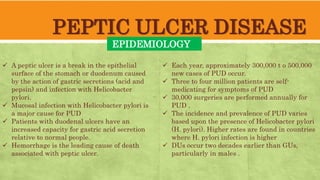
PEPTIC ULCER DISEASE
EPIDEMIOLOGY
Apeptic ulcer is a break in the epithelial
surface of the stomach or duodenum caused
by the action of gastric secretions (acid and
pepsin) and infection with Helicobacter
pylori.
Mucosal infection with Helicobacter pylori is
a major cause for PUD
Patients with duodenal ulcers have an
increased capacity for gastric acid secretion
relative to normal people.
Hemorrhage is the leading cause of death
associated with peptic ulcer.
Each year, approximately 300,000 t o 500,000
new cases of PUD occur.
Three to four million patients are self-
medicating for symptoms of PUD
30,000 surgeries are performed annually for
PUD .
The incidence and prevalence of PUD varies
based upon the presence of Helicobacter pylori
(H. pylori). Higher rates are found in countries
where H. pylori infection is higher
DUs occur two decades earlier than GUs,
particularly in males .
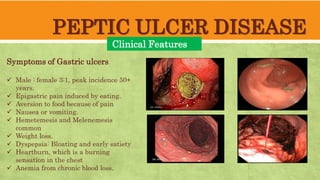
PEPTIC ULCER DISEASE
ClinicalFeatures
Symptoms of Gastric ulcers
Male : female 3:1, peak incidence 50+
years.
Epigastric pain induced by eating.
Aversion to food because of pain
Nausea or vomiting.
Hemetemesis and Melenemesis
common
Weight loss.
Dyspepsia: Bloating and early satiety
Heartburn, which is a burning
sensation in the chest
Anemia from chronic blood loss.
83.
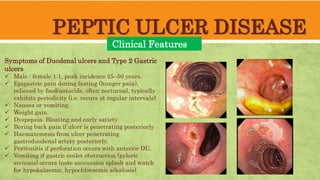
PEPTIC ULCER DISEASE
ClinicalFeatures
Symptoms of Duodenal ulcers and Type 2 Gastric
ulcers
Male : female 1:1, peak incidence 25–50 years.
Epigastric pain during fasting (hunger pain),
relieved by food/antacids, often nocturnal, typically
exhibits periodicity (i.e. recurs at regular intervals).
Nausea or vomiting.
Weight gain.
Dyspepsia: Bloating and early satiety
Boring back pain if ulcer is penetrating posteriorly
Haematemesis from ulcer penetrating
gastroduodenal artery posteriorly.
Peritonitis if perforation occurs with anterior DU.
Vomiting if gastric outlet obstruction (pyloric
stenosis) occurs (note succussion splash and watch
for hypokalaemic, hypochloraemic alkalosis).
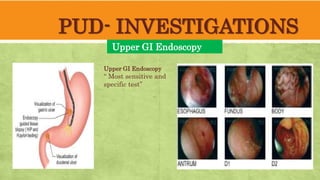
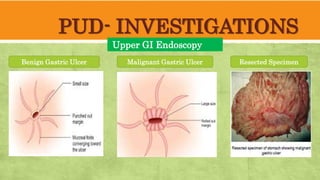
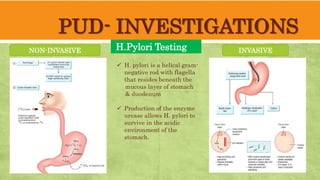
PUD- INVESTIGATIONS
H.Pylori Testing
NON-INVASIVEINVASIVE
H. pylori is a helical gram-
negative rod with flagella
that resides beneath the
mucous layer of stomach
& duodenum
Production of the enzyme
urease allows H. pylori to
survive in the acidic
environment of the
stomach.
88.
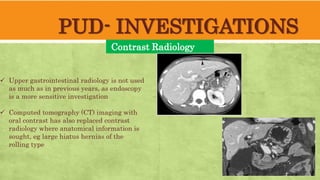
PUD- INVESTIGATIONS
Contrast Radiology
Uppergastrointestinal radiology is not used
as much as in previous years, as endoscopy
is a more sensitive investigation
Computed tomography (CT) imaging with
oral contrast has also replaced contrast
radiology where anatomical information is
sought, eg large hiatus hernias of the
rolling type
89.
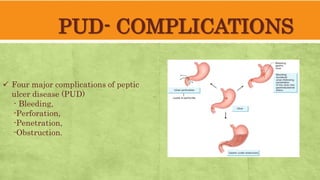
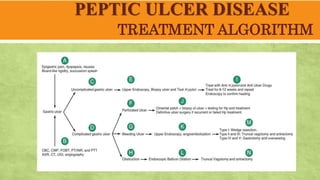
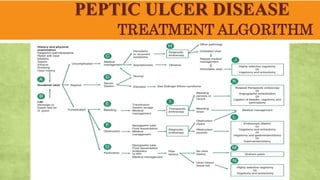
PUD- COMPLICATIONS
Four majorcomplications of peptic
ulcer disease (PUD)
- Bleeding,
-Perforation,
-Penetration,
-Obstruction.
90.
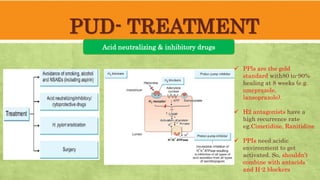
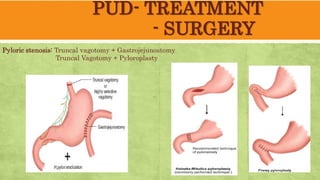
PUD- TREATMENT
PPls arethe gold
standard with80 to-90%
healing at 8 weeks (e.g.
omeprazole,
lansoprazole).
H2 antagonists have a
high recurrence rate
eg.Cimetidine, Ranitidine
PPIs need acidic
environment to get
activated. So, shouldn’t
combine with antacids
and H-2 blockers
Acid neutralizing & inhibitory drugs
91.
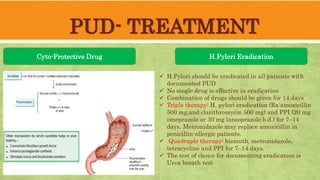
PUD- TREATMENT
Cyto-Protective DrugH.Pylori Eradication
H.Pylori should be eradicated in all patients with
documented PUD
No single drug is effective in eradication
Combination of drugs should be given for 14 days
Triple therapy: H. pylori eradication (Rx:amoxicillin
500 mg,and clarithromycin 500 mg) and PPI (20 mg
omeprazole or 30 mg lansoprazole b.d.) for 7–14
days. Metronidazole may replace amoxicillin in
penicillin-allergic patients.
Quadruple therapy: bismuth, metronidazole,
tetracycline and PPI for 7–14 days.
The test of choice for documenting eradication is
Urea breath test
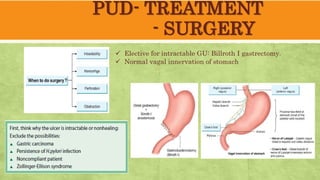
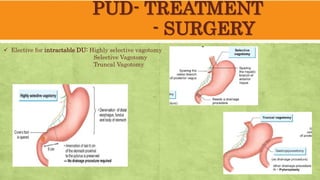
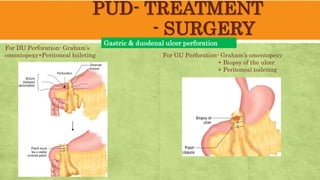
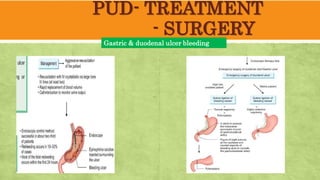
PUD- TREATMENT
- SURGERY
Gastric& duodenal ulcer perforation
For DU Perforation- Graham’s
omentopexy+Peritoneal toileting For GU Perforation- Graham’s omentopexy
+ Biopsy of the ulcer
+ Peritoneal toileting
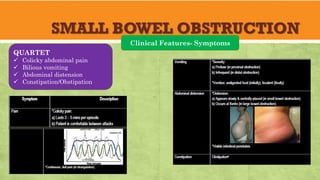
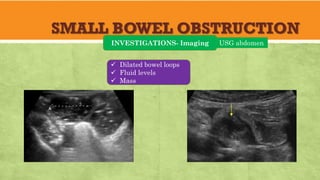
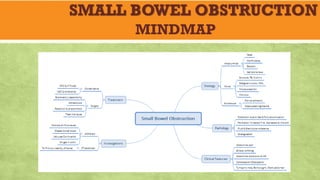
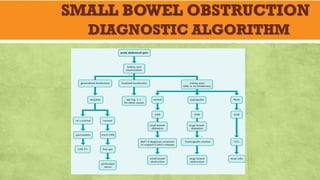
SMALL BOWEL OBSTRUCTION
Epidemiology
✓Stoppage of cranio- caudal propulsion of bowel
contents due to narrowing or complete
blockage of bowel lumen.
✓ Common surgical emergency, serious in nature
and demands early diagnosis and intervention
✓ SBO is more common and more severe than
LBO
✓ Post-op adhesion and obstructed inguinal
hernia are the two common causes
✓ The prevalence of small bowel obstruction is
approximately 100 - 500 per 100,000 - who
have not undergone previous abdominal
surgery.
✓ The prevalence of small bowel obstruction is
approximately 600 per 100,000 in patients who
have undergone previous abdominal surgery
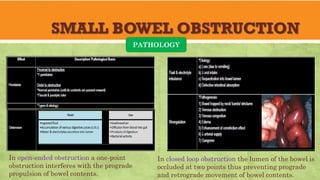
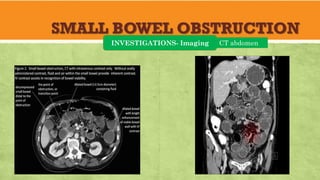
SMALL BOWEL OBSTRUCTION
PATHOLOGY
Inopen-ended obstruction a one-point
obstruction interferes with the prograde
propulsion of bowel contents.
In closed loop obstruction the lumen of the bowel is
occluded at two points thus preventing prograde
and retrograde movement of bowel contents.
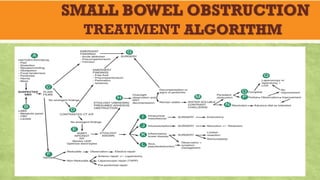
SMALL BOWEL OBSTRUCTION
TREATMENT
Signsof recuperation:
✓ Relief from symptoms (pain & vomiting)
✓ Improvement of general condition & vitals
✓ Amount of aspirate ↓
✓ Abdominal girth ↓
✓ Return of bowel sounds
• Conservative management can be continued
if above are present
Indications for early surgical intervention
✓ Obstructed external hernia
✓ Clinical features suspicious of intestinal
strangulation
✓ Obstruction in a ‘virgin’ abdomen
Principles of surgical intervention for
obstruction
Management of:
✓ The segment at the site of obstruction
✓ The distended proximal bowel
✓ The underlying cause of obstruction
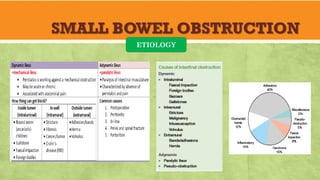
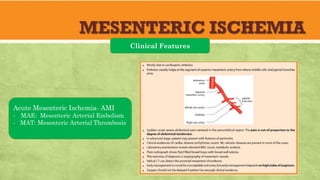
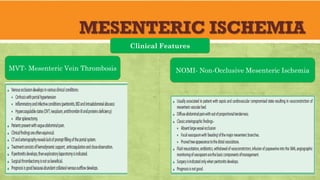
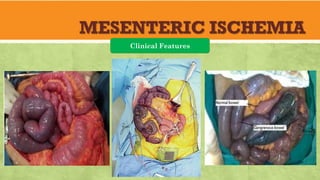
MESENTERIC ISCHEMIA
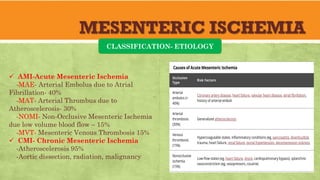
CLASSIFICATION- ETIOLOGY
AMI-Acute Mesenteric Ischemia
-MAE- Arterial Embolus due to Atrial
Fibrillation- 40%
-MAT- Arterial Thrombus due to
Atheroscelerosis- 30%
-NOMI- Non-Occlusive Mesenteric Ischemia
due low volume blood flow – 15%
-MVT- Mesenteric Venous Thrombosis 15%
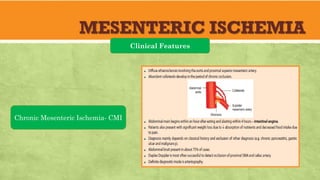
CMI- Chronic Mesenteric Ischemia
-Atheroscelerosis 95%
-Aortic dissection, radiation, malignancy
129.
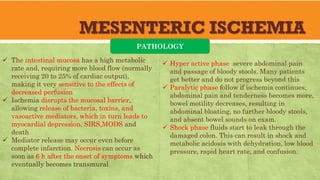
MESENTERIC ISCHEMIA
PATHOLOGY
Theintestinal mucosa has a high metabolic
rate and, requiring more blood flow (normally
receiving 20 to 25% of cardiac output),
making it very sensitive to the effects of
decreased perfusion
Ischemia disrupts the mucosal barrier,
allowing release of bacteria, toxins, and
vasoactive mediators, which in turn leads to
myocardial depression, SIRS,MODS and
death
Mediator release may occur even before
complete infarction. Necrosis can occur as
soon as 6 h after the onset of symptoms which
eventually becomes transmural
Hyper active phase severe abdominal pain
and passage of bloody stools. Many patients
get better and do not progress beyond this
Paralytic phase follow if ischemia continues;
abdominal pain and tenderness becomes more,
bowel motility decreases, resulting in
abdominal bloating, no further bloody stools,
and absent bowel sounds on exam.
Shock phase fluids start to leak through the
damaged colon. This can result in shock and
metabolic acidosis with dehydration, low blood
pressure, rapid heart rate, and confusion.
130.
MESENTERIC ISCHEMIA
EPIDEMIOLOOGY
Mesentericischemia is insufficient perfusion
of the mesentery to meet the metabolic
demands of the splanchnic system.
Prompt diagnosis and treatment of this life-
threatening condition, with mortality rates
from 24% to 94% is important
Despite the best efforts of modern medicine
mortality still exceeds 50%
Acute mesenteric ischemia is different from
ischemic colitis, which involves only small
vessels and causes mainly mucosal necrosis
and bleeding.
The overall incidence for Mesenteric Ischemia
is estimated at 12.9/100,000 person/year
Incidence of Acute superior mesenteric artery
(SMA) occlusion (embolus/thrombus ratio =
1.4) is 70%
Incidence of Mesenteric venous thrombosis
(MVT) is 15%
Nonocclusive mesenteric ischemia (NOMI)
were found in 15%
MESENTERIC ISCHEMIA
INESTIGATIONS- LABS
White blood cell count >10.5 in 98%
Lactic acid elevated 91%
In very early stage these two may not be elevated
However, in late cases both are elevated
136.
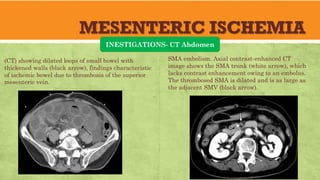
MESENTERIC ISCHEMIA
INESTIGATIONS- CTAbdomen
SMA embolism. Axial contrast-enhanced CT
image shows the SMA trunk (white arrow), which
lacks contrast enhancement owing to an embolus.
The thrombosed SMA is dilated and is as large as
the adjacent SMV (black arrow).
(CT) showing dilated loops of small bowel with
thickened walls (black arrow), findings characteristic
of ischemic bowel due to thrombosis of the superior
mesenteric vein.
137.
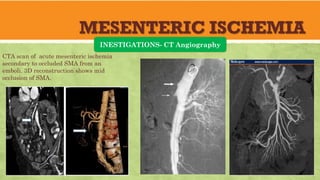
MESENTERIC ISCHEMIA
INESTIGATIONS- CTAngiography
CTA scan of acute mesenteric ischemia
secondary to occluded SMA from an
emboli. 3D reconstruction shows mid
occlusion of SMA.
138.
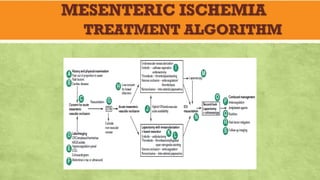
MESENTERIC ISCHEMIA
TREATMENT
Acute MesentericIschemia:
If diagnosis is made during exploratory laparotomy, options
are surgical embolectomy, revascularization, and resection.
A “second look” laparotomy may be needed to reassess the
viability of questionable areas of bowel.
Patients with arterial embolism or venous thrombosis require
long-term anticoagulation with warfarin. Patients with
nonocclusive ischemia may be treated with antiplatelet
therapy.
139.
MESENTERIC ISCHEMIA
TREATMENT
Chronic MesentericIschemia:
If diagnosis is made by angiography, infusion of
the vasodilator papaverine through the
angiography catheter may improve survival in both
occlusive and nonocclusive ischemia
For arterial thrombosis, Catheter directed
thrombolysis, balloon angioplasty or surgical by-
pass surgery may be done
Mesenteric venous thrombosis without signs of
peritonitis can be treated with papaverine followed
by anticoagulation with heparin and then
warfarin.
140.
MESENTERIC ISCHEMIA
TAKE HOMEMESSAGE
Early diagnosis is critical because mortality increases significantly once
intestinal infarction has occurred.
Initially, pain is severe but physical findings are minimal- Pain out of
proportion to physical findings
Surgical exploration is often the best diagnostic measure for patients with
definite peritoneal signs.
For other patients, mesenteric angiography or CT angiography is done.
For AMI embolectomy, revascularization, and resection.
For CMI thrombolysis, angioplasty or by-pass surgery
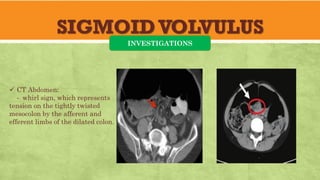
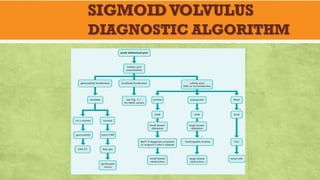
SIGMOIDVOLVULUS
Epidemiology
✓ Volvulus occurswhen a segment of colon
undergoes twisting along its own mesentery
(mesenterio-axial) resulting in obstruction.
✓ Twisting of 180 degrees results in clinical
obstruction, and further twisting to 360
degrees causes strangulation with venous
gangrene, ischemia, and eventual perforation.
✓ It is a closed loop obstruction
✓ Common in elderly and those who are taking
neuro-psychiatric drugs
✓ Sigmoid volvulus accounts for 5% of large
bowel obstruction in developed countries. and
10% to 50% in developing countries
✓ This is because of intake of high-fibre diet in
these countries
✓ Patients are often institutionalized and
debilitated due to underlying neurologic or
psychiatric disease and have a history of
constipation
148.
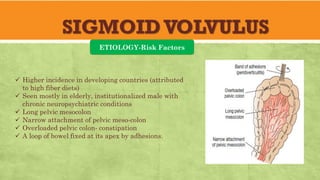
SIGMOIDVOLVULUS
ETIOLOGY-Risk Factors
✓ Higherincidence in developing countries (attributed
to high fiber diets)
✓ Seen mostly in elderly, institutionalized male with
chronic neuropsychiatric conditions
✓ Long pelvic mesocolon
✓ Narrow attachment of pelvic meso-colon
✓ Overloaded pelvic colon- constipation
✓ A loop of bowel fixed at its apex by adhesions.
149.
SIGMOIDVOLVULUS
PATHOLOGY
✓ The loopof sigmoid colon usually
undergoes twisting in an
anticlockwise direction from one
half to three turns.
✓ As the volvulized segment
enlarges, it becomes trapped in the
confines of the abdominal wall and
is unable to spontaneously detorse.
150.
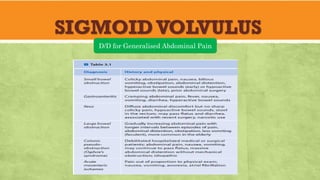
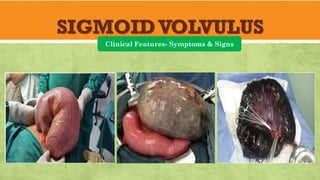
SIGMOIDVOLVULUS
Clinical Features- Symptoms& Signs
SYMPTOMS
✓ Abdominal pain (initially
left-sided, later diffuse)
✓ Enormous abdominal
distension (left iliac fossa
and then whole of abdomen)
✓ Obstipation
✓ Hiccough, retching
✓ Vomiting- late feature
SIGNS
✓ Tympanic abdomen
✓ Tyre-like consistency of abdomen
is diagnostic
✓ Empty rectal vault (on digital
rectal exam)
✓ Just distension of abdomen
without tenderness→Viable
bowel
✓ Generalised tenderness with
rebound tenderness→
Gangrenous bowel
✓ Rigid abdomen→ Bowel
perforation
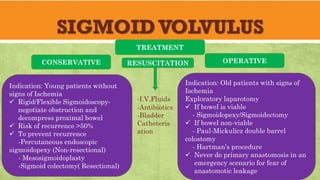
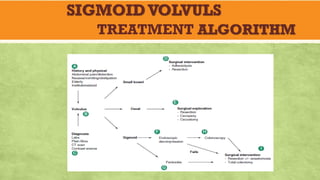
SIGMOIDVOLVULUS
TREATMENT
Indication: Young patientswithout
signs of Ischemia
✓ Rigid/Flexible Sigmoidoscopy-
negotiate obstruction and
decompress proximal bowel
✓ Risk of recurrence >50%
✓ To prevent recurrence
-Percutaneous endoscopic
sigmoidopexy (Non-resectional)
- Mesosigmoidoplasty
-Sigmoid colectomy( Resectional)
Indication: Old patients with signs of
Ischemia
Exploratory laparotomy
✓ If bowel is viable
- Sigmoidopexy/Sigmoidectomy
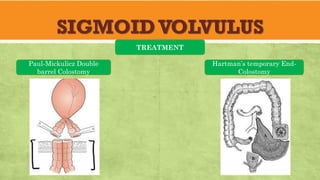
✓ If bowel non-viable
- Paul-Mickulicz double barrel
colostomy
- Hartman’s procedure
✓ Never do primary anastomosis in an
emergency scenario for fear of
anastomotic leakage
CONSERVATIVE OPERATIVE
RESUSCITATION
-I.V.Fluids
-Antibiotics
-Bladder
Catheteris
ation