Tuberculosis is a chronic granulomatous disease caused by Mycobacterium species as, Mycobacterium tuberculosis- in human
Mycobacterium bovis- in animals
Mycobacterium leprae- cause leprosy
Global Emergency Tuberculosis kills 5000 people a day.
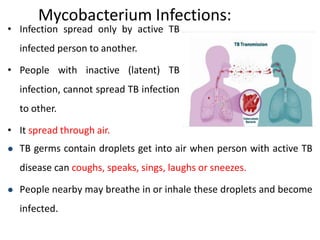
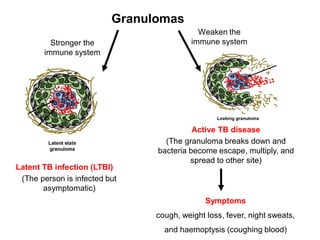
Infection spread only by active TB infected person to another.
People with inactive (latent) TB infection, cannot spread TB infection to other.

![Pyrazinamide (PZA]
• pyrazine-2-carboxamide
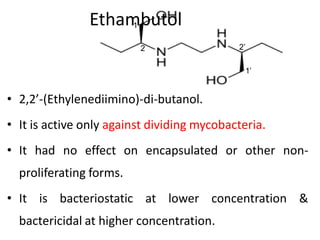
• It is active only against dividing mycobacteria.
• It had no effect on encapsulated or other non-
proliferating forms.
• Prodrug](https://image.slidesharecdn.com/anti-tbagents-260210022354-63083bc3/85/Antitubercular-agents-medicinal-chemistry-pdf-24-320.jpg)
![Newer Drug
Rifabutin
• Semi-Synthetic derivative of rifamycin B.
8-isobutyl-1,4,8-triazaspiro[4.5]dec-1-ene
Spiroimidazopiperidyl
derivative
two rings that share a
single atom.](https://image.slidesharecdn.com/anti-tbagents-260210022354-63083bc3/85/Antitubercular-agents-medicinal-chemistry-pdf-30-320.jpg)
![P-Amino Salicylic Acid (PAS)
• MOA: It's structural similarity with PABA. Therefore it prevent the
incorporation of PABA into dihydrofolic acid molecule, catalysed by
the enzyme dihydrofolate synthatase, leads to block the synthesis
of folic acid.
• SAR: I] Amino & carboxylic gp. are must be para to each other &
free. II] –OH gp may at ortho or meta, but at ortho position shows
more efficiency.
• Adverse effects: Nausea, diarrhoea, loss of appetite,
agranulocytosis, haemolytic anaemia, and allergic reactions.](https://image.slidesharecdn.com/anti-tbagents-260210022354-63083bc3/85/Antitubercular-agents-medicinal-chemistry-pdf-38-320.jpg)


























![ANTI HYPERTENSIVE AGENTS [MEDICINAL CHEMISTRY] BY P.RAVISANKAR, HYPERTENSION,...](https://cdn.slidesharecdn.com/ss_thumbnails/antihypertensiveagents-ravi-130615193634-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)





