Download as PDF, PPTX

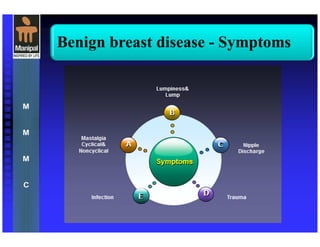
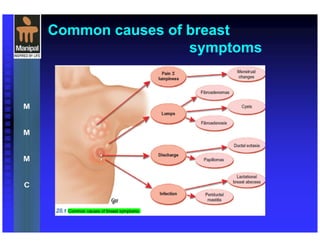



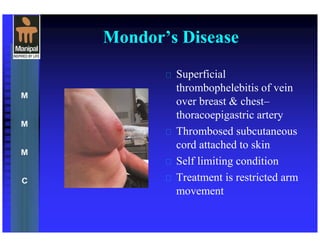

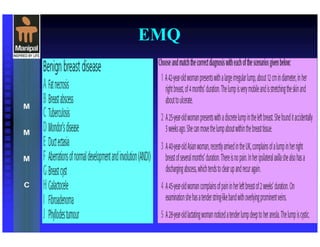
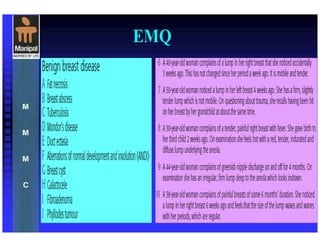


The document provides an extensive overview of benign breast diseases, detailing their symptoms, causes, and treatments. It covers various conditions such as mastalgia, fibrocystic disease, duct ectasia, galactocele, and breast abscesses, emphasizing the importance of diagnosis and management. The document also highlights that benign breast disorders are common and often present with lumps and pain, necessitating tailored treatment approaches.











































































































