Downloaded 118 times
![ Frequently include an anomalous junction of the
pancreatic duct and CBD (pancreaticobiliary
malunion [PBMU])
Intrahepatic bile duct dilatation with or without
downstream stenosis
Varying degrees of hepatic fibrosis](https://image.slidesharecdn.com/surgicaljaundiceinneonates7thyr-170109125953/85/Surgical-jaundice-in-neonates-35-320.jpg)

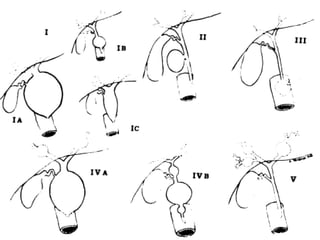

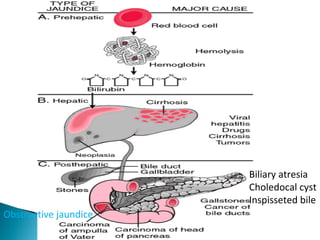
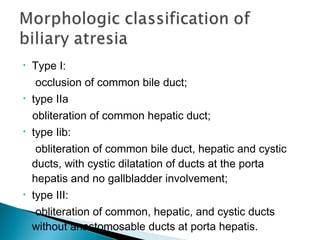
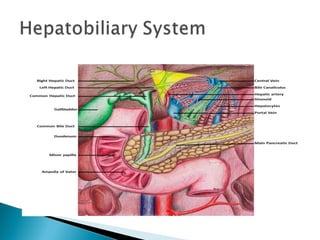
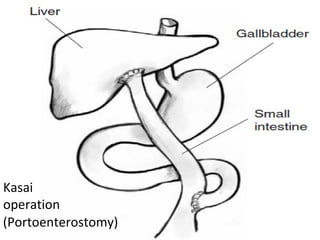
This document discusses various causes of obstructive jaundice in infants. It begins by describing the signs and symptoms of jaundice. It then categorizes the different types of jaundice that can occur in the first few weeks of life. The main causes discussed are biliary atresia, choledochal cysts, and inspissated bile. For each condition, the document outlines the pathogenesis, clinical features, diagnostic evaluation, and treatment options. It emphasizes that early surgical intervention is important for conditions like biliary atresia to prevent progression to liver damage and need for transplantation.




















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)















