OBSTRUCTIVE JAUNDICE- Problem Oriented Approach.pptx
Here discussing various cases of Obstructive jaundice namely Choledocholithiassis, Biliary atresia, Carcinoma Pancreas, Periampullary Carcinoma and Cholangiocarcinoma.
OBSTRUCTIVE JAUNDICE
Definition &Importance
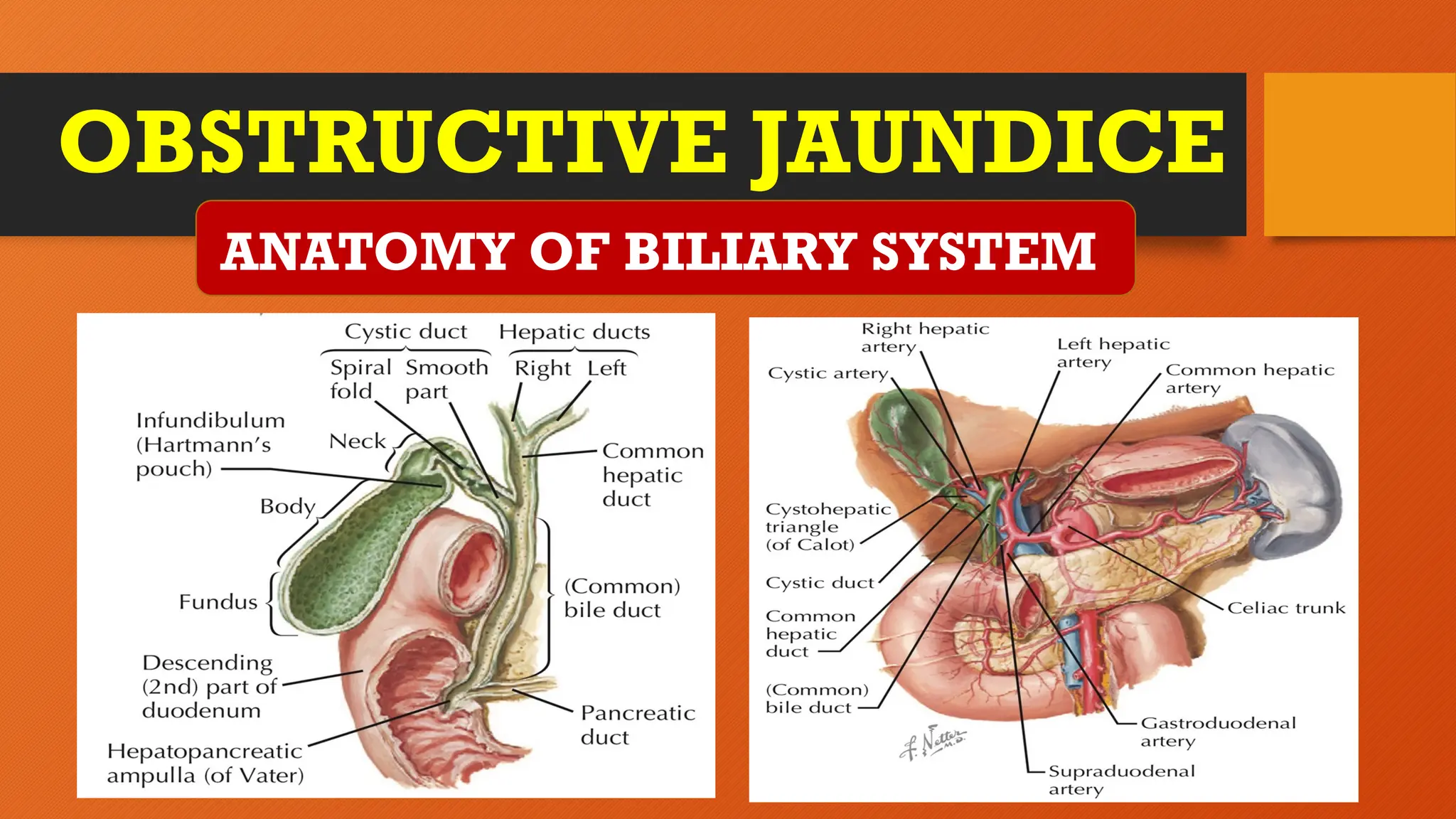
Anatomy of Biliary system
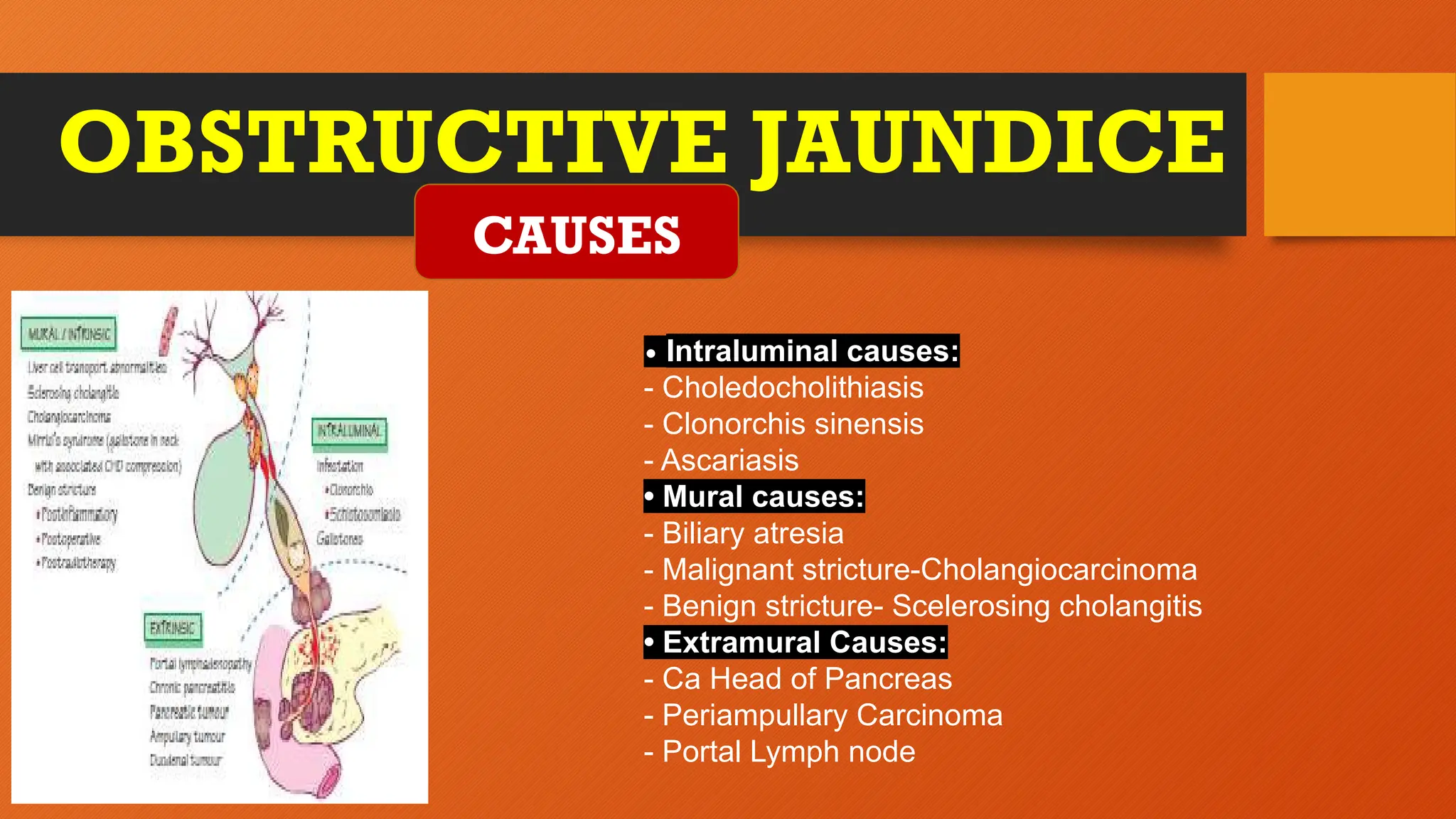
Causes of obstructive jaundice
Choledocholithiasis
Biliary Atresia
Carcinoma Head of the Pancreas
Periampullary Carcinoma
Cholangio Carcinoma
Quick recap/Conclusion
LEARNING OBJECTIVES
3.
OBSTRUCTIVE JAUNDICE
Definition: Obstructivejaundice is a medical
condition characterized by the obstruction of
normal bile flow from the liver to the small
intestine, leading to the accumulation of
bilirubin in the bloodstream. Bilirubin is a
yellow pigment formed during the breakdown
of red blood cells.
Implications of Untreated Obstructive
Jaundice: It can lead to progressive liver
damage with impaired bile secretion and
digestion
Definition & Importance
Timely Diagnosis for Effective Intervention:
Early diagnosis allows for prompt intervention,
preventing potential complications and improving the
chances of successful treatment.
Multidisciplinary Approach: The need for a
collaborative approach involving various healthcare
professionals, including gastroenterologists,
hepatologists, surgeons, and radiologists, to ensure
comprehensive care.
CHOLEDOCHOLITHIASIS
Etiopathogenesis Clinical Features-S&S Diagnosis- Workup Treatment
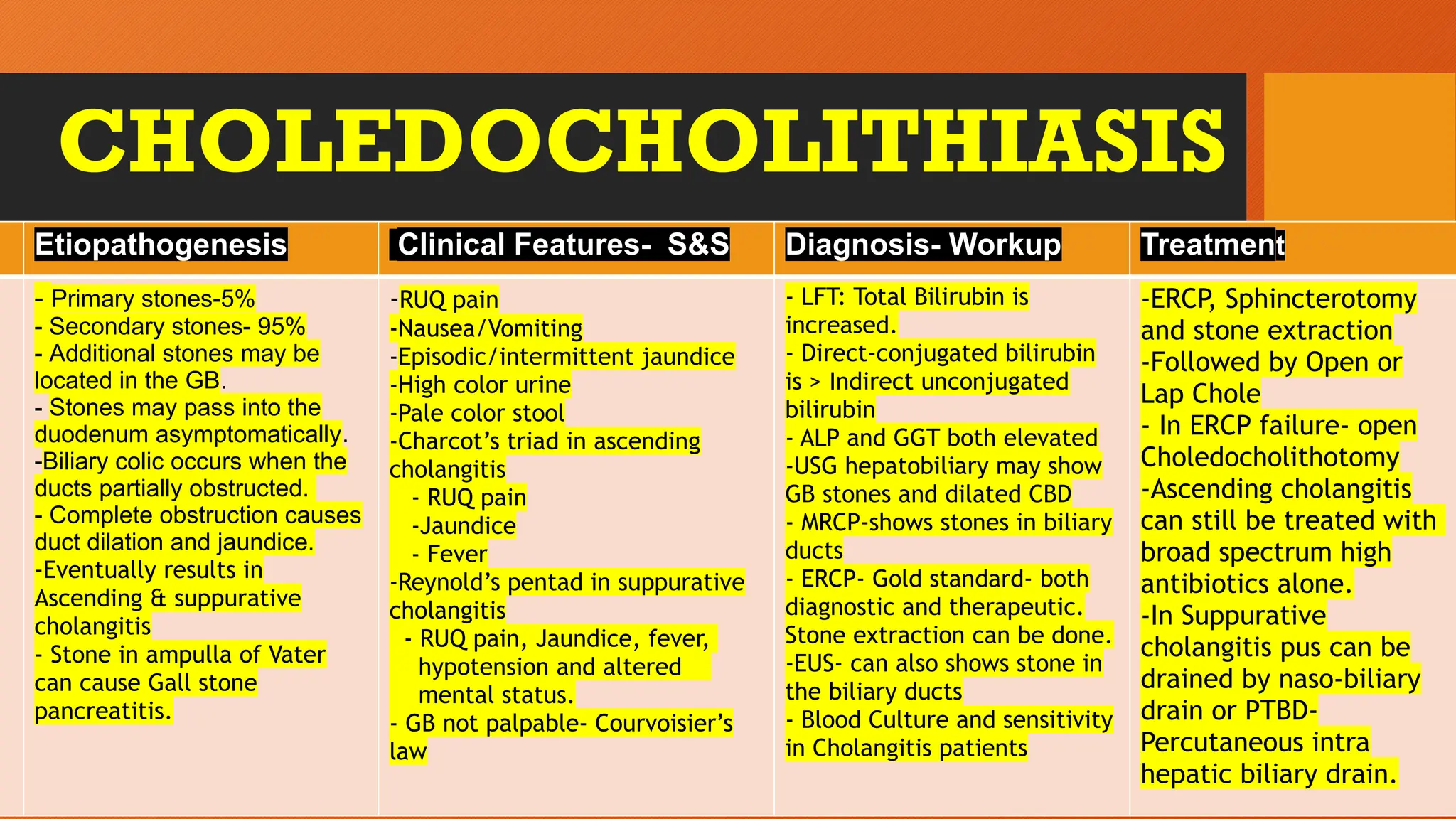
- Primary stones-5%
- Secondary stones- 95%
- Additional stones may be
located in the GB.
- Stones may pass into the
duodenum asymptomatically.
-Biliary colic occurs when the
ducts partially obstructed.
- Complete obstruction causes
duct dilation and jaundice.
-Eventually results in
Ascending & suppurative
cholangitis
- Stone in ampulla of Vater
can cause Gall stone
pancreatitis.
-RUQ pain
-Nausea/Vomiting
-Episodic/intermittent jaundice
-High color urine
-Pale color stool
-Charcot’s triad in ascending
cholangitis
- RUQ pain
-Jaundice
- Fever
-Reynold’s pentad in suppurative
cholangitis
- RUQ pain, Jaundice, fever,
hypotension and altered
mental status.
- GB not palpable- Courvoisier’s
law
- LFT: Total Bilirubin is
increased.
- Direct-conjugated bilirubin
is > Indirect unconjugated
bilirubin
- ALP and GGT both elevated
-USG hepatobiliary may show
GB stones and dilated CBD
- MRCP-shows stones in biliary
ducts
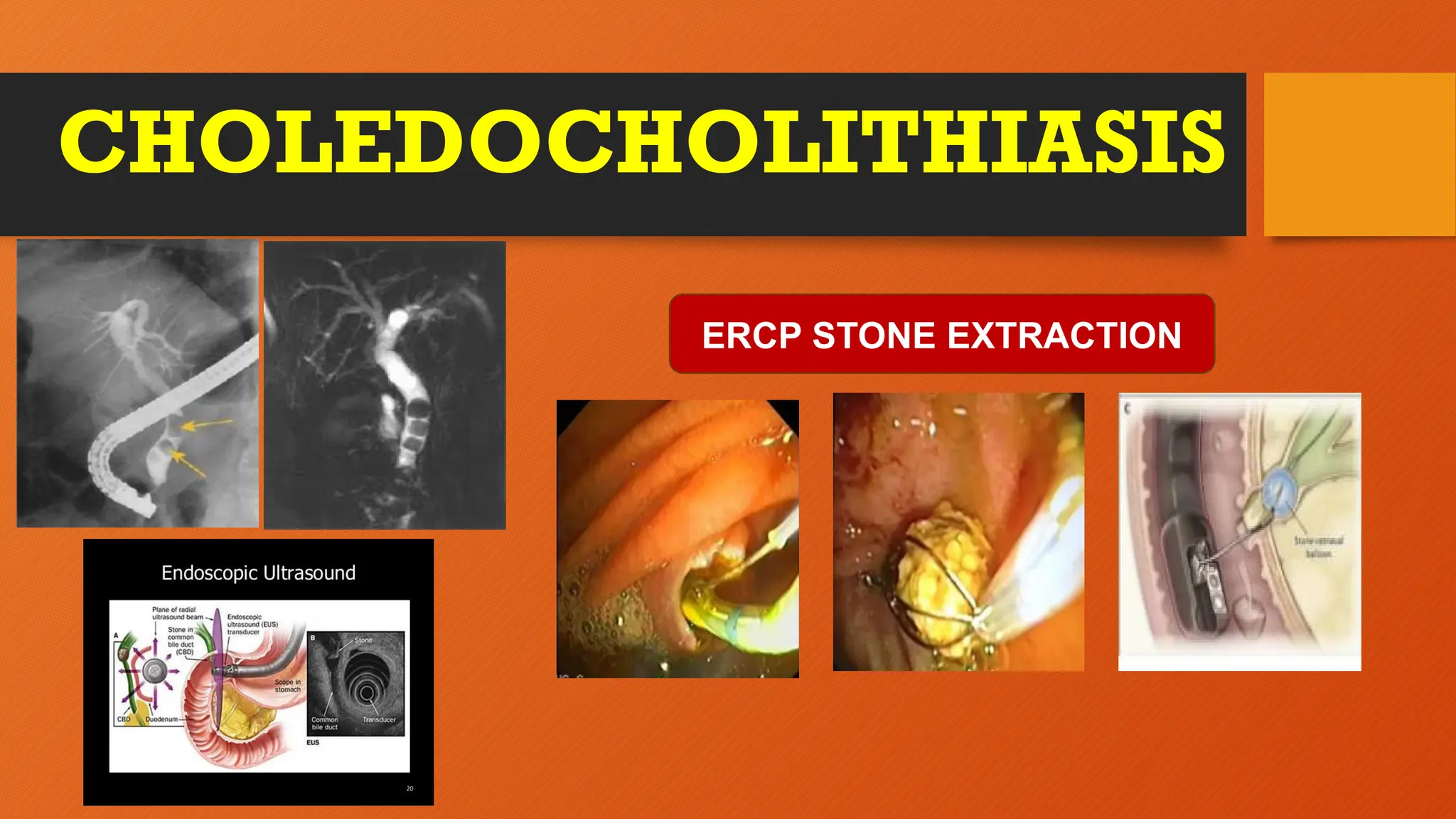
- ERCP- Gold standard- both
diagnostic and therapeutic.
Stone extraction can be done.
-EUS- can also shows stone in
the biliary ducts
- Blood Culture and sensitivity
in Cholangitis patients
-ERCP, Sphincterotomy
and stone extraction
-Followed by Open or
Lap Chole
- In ERCP failure- open
Choledocholithotomy
-Ascending cholangitis
can still be treated with
broad spectrum high
antibiotics alone.
-In Suppurative
cholangitis pus can be
drained by naso-biliary
drain or PTBD-
Percutaneous intra
hepatic biliary drain.
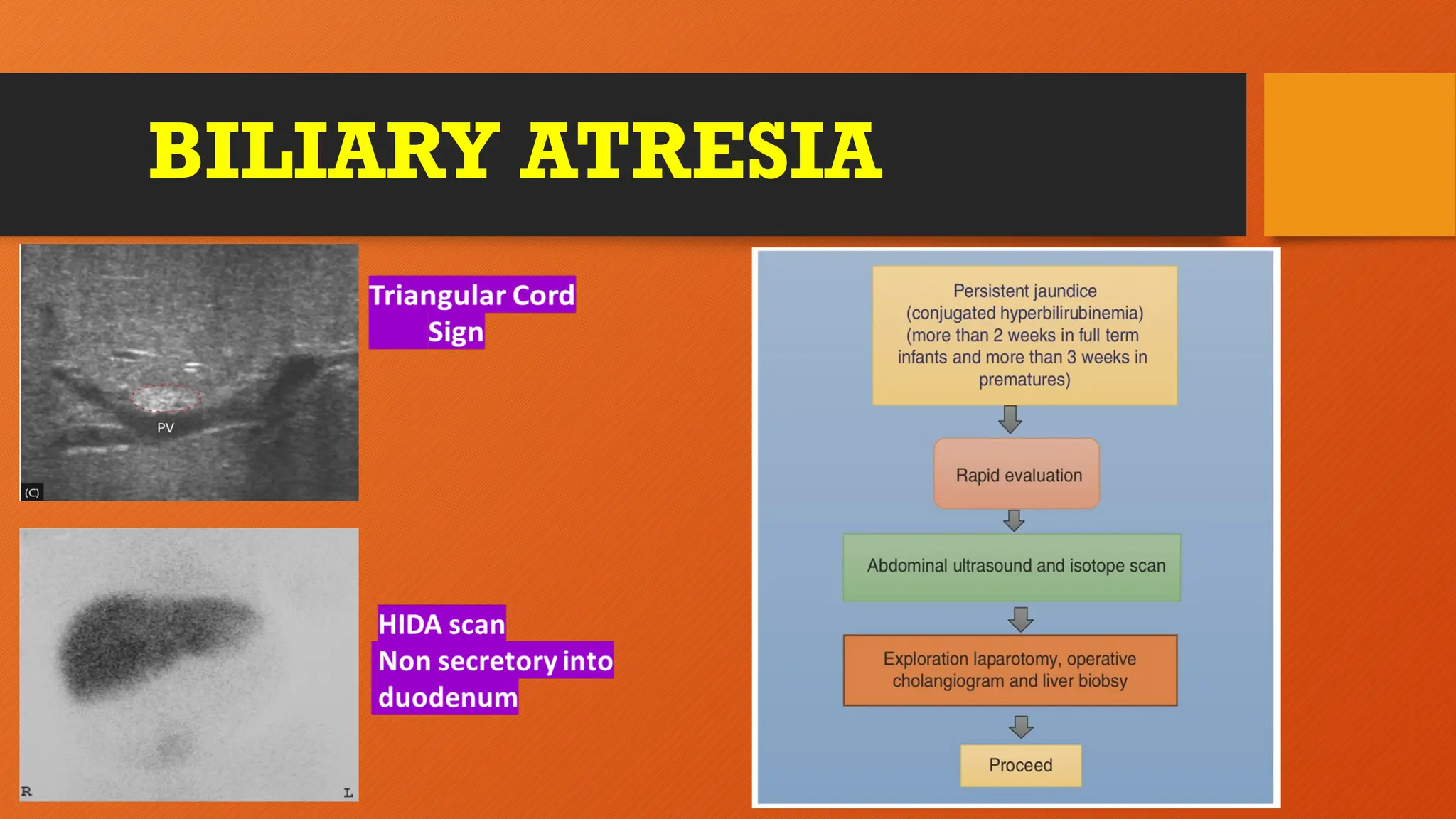
BILIARY ATRESIA
Etiopathogenesis ClinicalFeatures- S&S Diagnosis- Workup Treatment
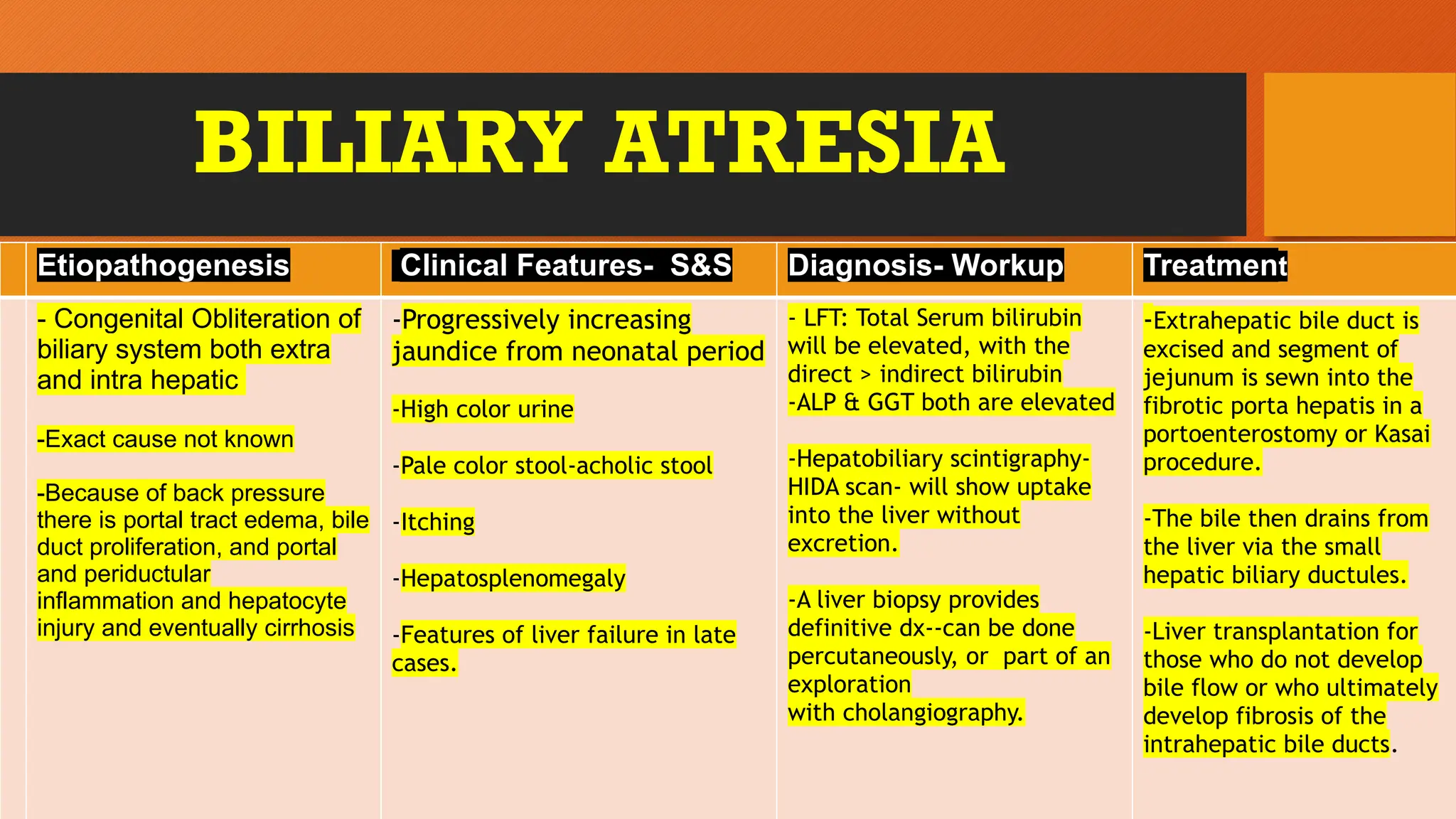
- Congenital Obliteration of
biliary system both extra
and intra hepatic
-Exact cause not known
-Because of back pressure
there is portal tract edema, bile
duct proliferation, and portal
and periductular
inflammation and hepatocyte
injury and eventually cirrhosis
-Progressively increasing
jaundice from neonatal period
-High color urine
-Pale color stool-acholic stool
-Itching
-Hepatosplenomegaly
-Features of liver failure in late
cases.
- LFT: Total Serum bilirubin
will be elevated, with the
direct > indirect bilirubin
-ALP & GGT both are elevated
-Hepatobiliary scintigraphy-
HIDA scan- will show uptake
into the liver without
excretion.
-A liver biopsy provides
definitive dx--can be done
percutaneously, or part of an
exploration
with cholangiography.
-Extrahepatic bile duct is
excised and segment of
jejunum is sewn into the
fibrotic porta hepatis in a
portoenterostomy or Kasai
procedure.
-The bile then drains from
the liver via the small
hepatic biliary ductules.
-Liver transplantation for
those who do not develop
bile flow or who ultimately
develop fibrosis of the
intrahepatic bile ducts.
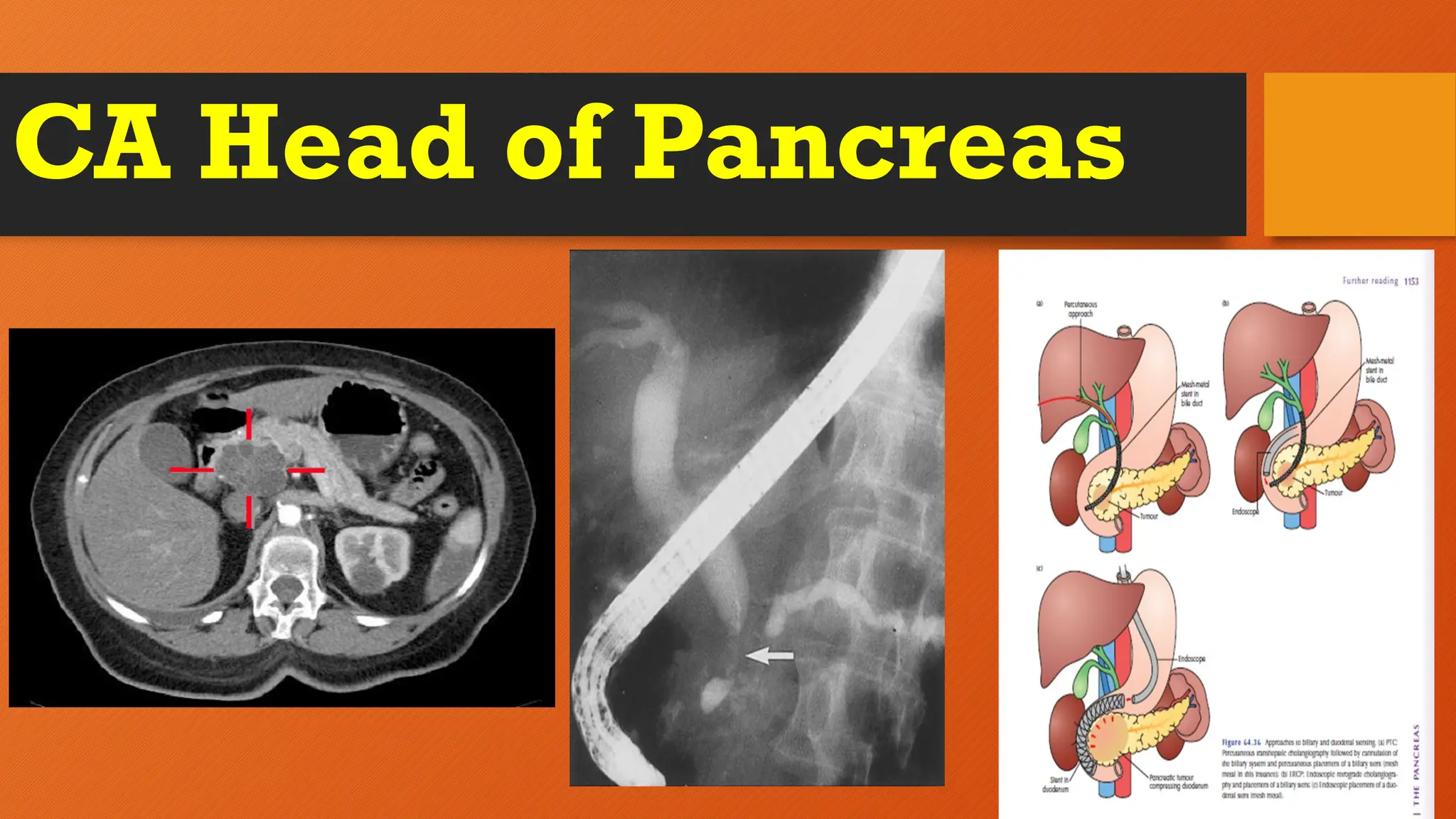
CA Head ofPancreas
Etiopathogenesis Clinical Features- S&S Diagnosis- Workup Treatment
- Exact cause not known
-Risk factors are Cigarette
smoking, Increased age.
Chronic pancreatitis, increased
saturated fat intake, exposure
to non chlorinated solvents
-Genetic risk factors- Chronic
familial relapsing pancreatitis,
Familial breast cancer BRCA2,
Gardener syndrome, HNPCC ,
Peutz-Jegher’s syndrome
-Tumor in the head of
Pancreas cause extrinsic
compression of distal CBD
causing Obstructive jaundice.
-Painless progressive jaundice
-High color urine
-Pale color stool-acholic stool
-Itching
-Nausea/vomiting
- Loss of weight and loss of
appetite
-Palpable GB- “Courvoisier’s Law”
-
- LFT: Total Serum bilirubin
will be elevated, with the
direct > indirect bilirubin
-ALP & GGT both are elevated
-ERCP- Dual duct sign
-USG Abd : can detect only
huge tumors
-Triple phase CT abdomen: is
sensitive to pickup even small
hypodense lesions and for
staging
-EUS- EUS guided pancreatic
biopsy
-Resectable tumors- tumors
confined to pancreas- Whipple’s
operation or
Pancreatoduodenectomy
-Borderline tumors-
Neoadjuvant chemoradio and
then surgery
-Unresectable tumors- only
palliative by pass surgeries
Biliary obstruction:
Biliary enteric bypass,
Endoscopic biliary stent
placement. Radiographic
transhepatic stent placement.
GOO- Gastroenteric bypass,
Endoscopically placed duodenal
stent
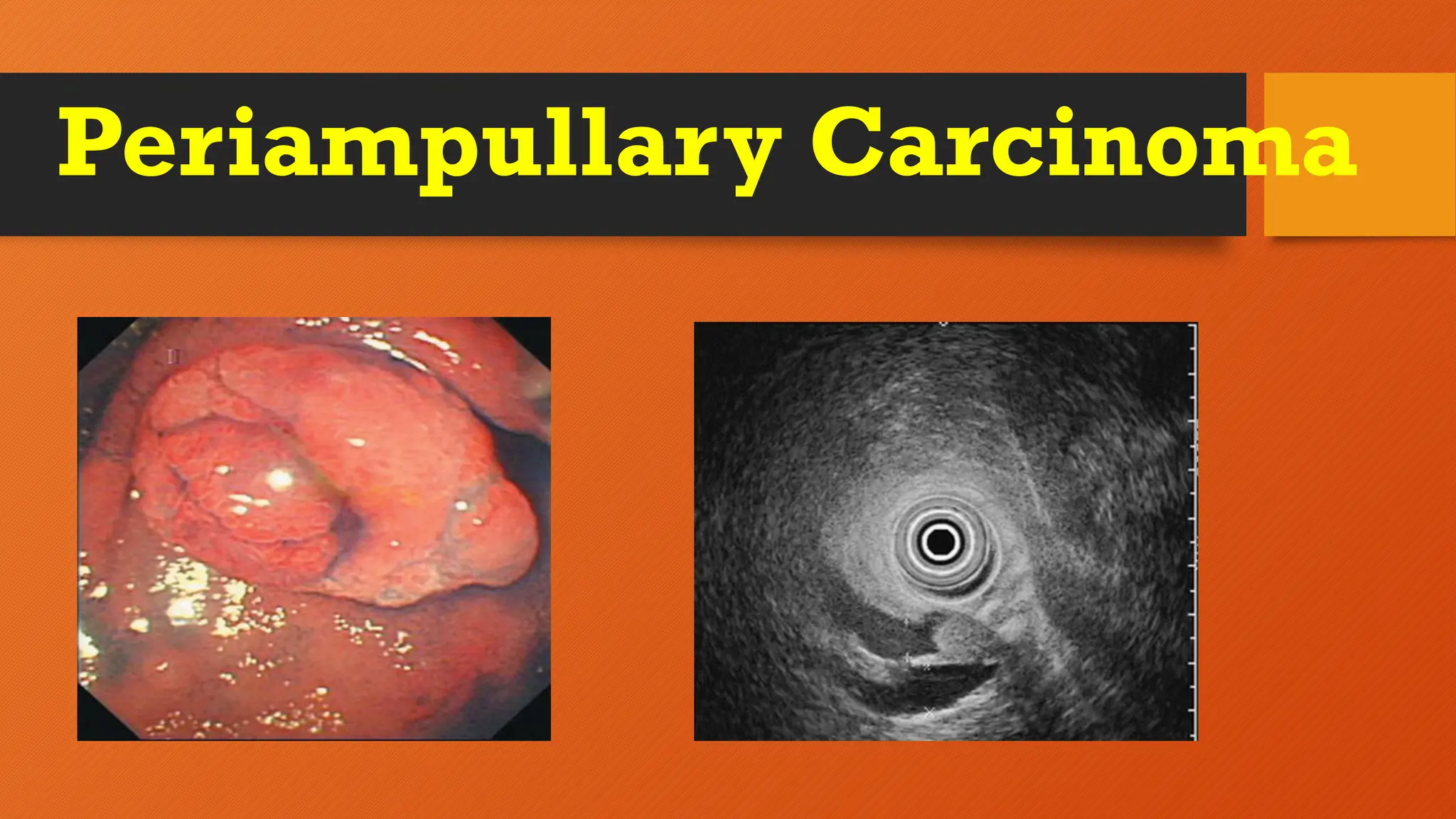
Periampullary Carcinoma
Etiopathogenesis ClinicalFeatures- S&S Diagnosis- Workup Treatment
- A malignant tumor arising
in the last centimeter of the
common bile duct.
-can arise from 1 of 4
epithelial types: Terminal
CBD, Duodenal mucosa,
Pancreatic duct and
Ampulla of Vater
-Ampullary adenocarcinomas
have two principal histologic
forms: intestinal and
pancreaticobiliary
-Pancreaticobiliary tumors
follow a more aggressive
course
-Painful intermittent jaundice
because of partial necrosis of
tumor
-High color urine
-Silver color stool-because of
mixing of blood oozing from the
tumor with acholic stool
-Itching
-Nausea/vomiting
- Loss of weight and loss of
appetite
-Palpable GB- “Courvoisier’s Law”
-Upper GI bleed & heme positive
stools—May occur due to
ulceration of ampullary mass (less
common)
-
- LFT: Total Serum bilirubin
will be elevated, with the
direct > indirect bilirubin
-ALP & GGT both are elevated
- CA 19-9 and CEA Serum
tumor markers elevated
-CT scan often demonstrates a
mass
-ERCP- to evaluate the ductal
architecture further
-EUS- EUS guided biopsy
-PET-CT scans can detect
metastases
-Resectable tumors: Whipple’s
operation or
Pancreatoduodenectomy
-Followed by adjuvant
chemotherapy
-Unresectable tumors- only
palliative by pass surgeries
Biliary obstruction:
Biliary enteric bypass,
Endoscopic biliary stent
placement. Radiographic
transhepatic stent placement.
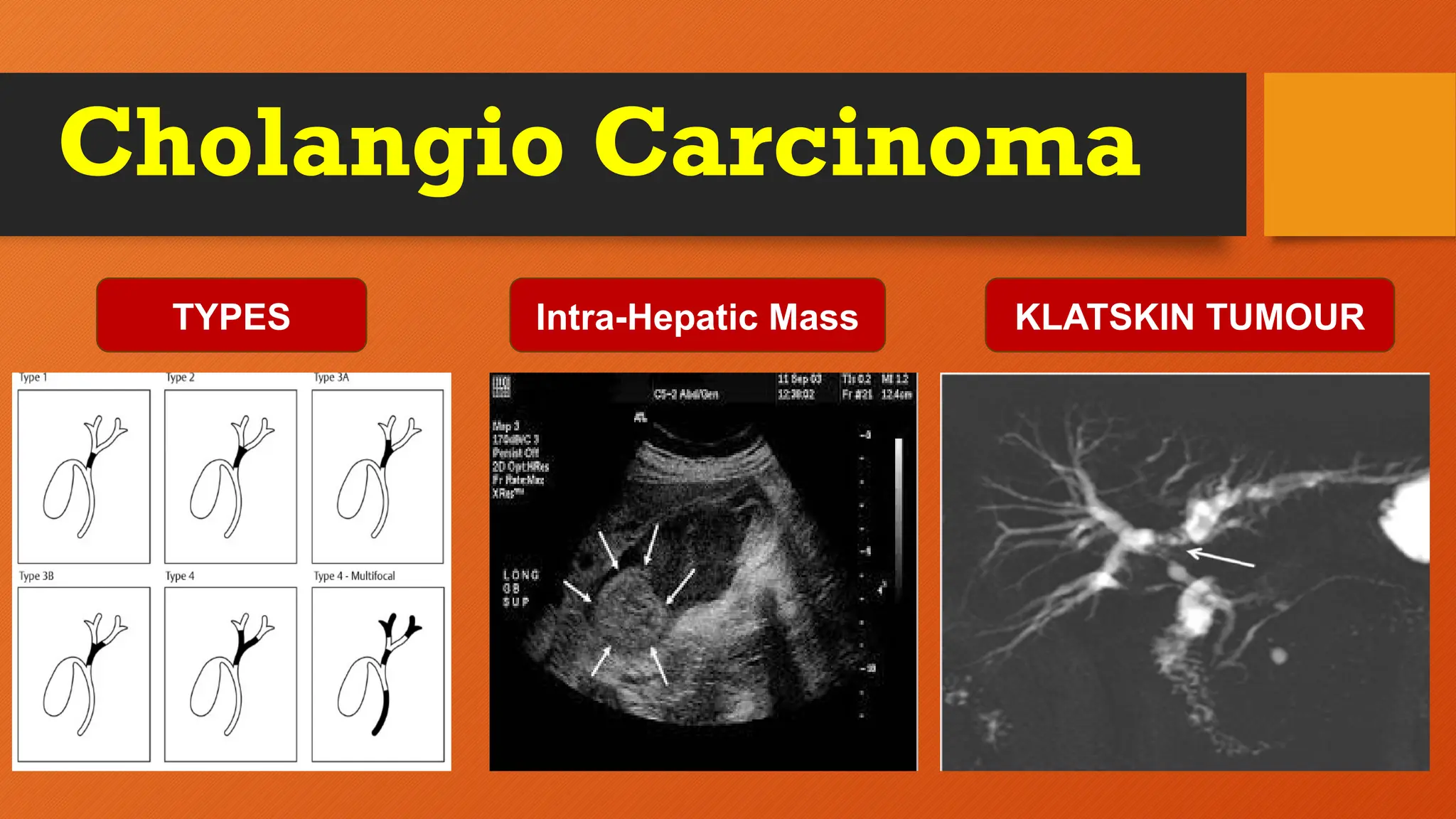
Cholangio Carcinoma
Etiopathogenesis ClinicalFeatures- S&S Diagnosis- Workup Treatment
- A malignant tumor arising
from intrahepatic or
extrahepatic bile ducts
-Extrahepatic is perihilar or
distal duct. Perihilar is
Klatskin tumor which is
very common
-Risk factors are Primary
scelerosing cholangitis or liver
flukes like Clonorchis sinensis
-Painful progressive jaundice
because of slow narrowing of
the duct
-High color urine
-Pale color stool
-Itching
-Nausea/vomiting
- Loss of weight and loss of
appetite
-Palpable GB- “Courvoisier’s Law”
-
- LFT: Total Serum bilirubin
will be elevated, with the
direct > indirect bilirubin
-ALP & GGT both are elevated
- In prolonged obstruction PT
is elevated because of VitK
malabsorption
- USG shows biliary duct
dilatation and larger hilar
lesions
-CT scan often demonstrates a
mass
-ERCP- shows site of
obstruction and for brush
cytology&palliative stenting
-EUS- EUS guided biopsy-FNAC
-PET-CT scans can detect
metastases
-Majority of tumors are
unresectable and complte
surgical excision is not possible.
-So, only the following
palliative treatment only can
be done
-ERCP and stenting
- PDT-Photodynamic Therapy
-Radiation therapy
-Chemotherapy
-Radiofrequency ablation
- Targeted therapy with
Futibatinib & Pemigatinib
CAUSES Etiopathogenesis ClinicalFeatures-
S&S
DIAGNOSIS TREATMENT
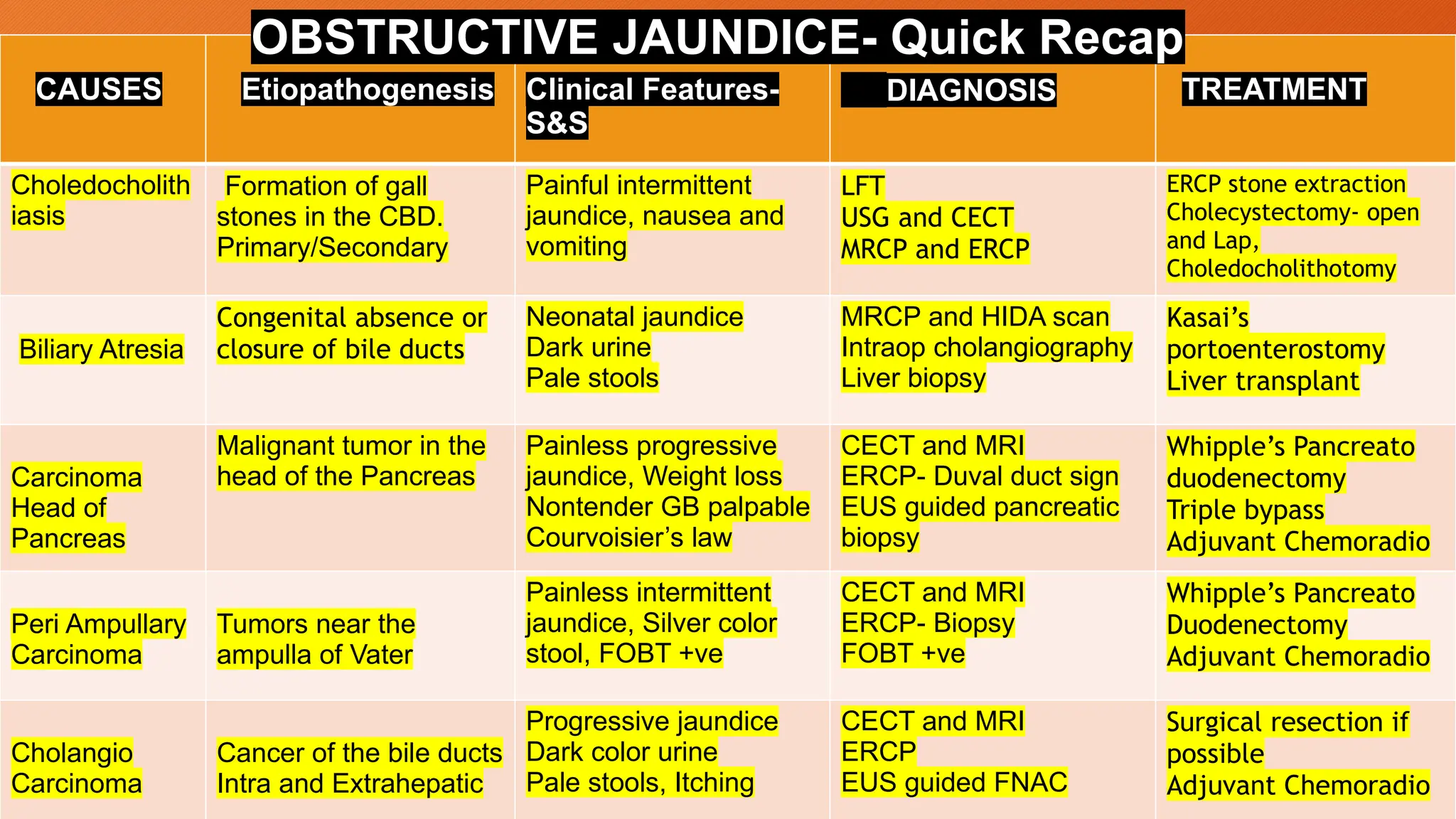
Choledocholith
iasis
Formation of gall
stones in the CBD.
Primary/Secondary
Painful intermittent
jaundice, nausea and
vomiting
LFT
USG and CECT
MRCP and ERCP
ERCP stone extraction
Cholecystectomy- open
and Lap,
Choledocholithotomy
Biliary Atresia
Congenital absence or
closure of bile ducts
Neonatal jaundice
Dark urine
Pale stools
MRCP and HIDA scan
Intraop cholangiography
Liver biopsy
Kasai’s
portoenterostomy
Liver transplant
Carcinoma
Head of
Pancreas
Malignant tumor in the
head of the Pancreas
Painless progressive
jaundice, Weight loss
Nontender GB palpable
Courvoisier’s law
CECT and MRI
ERCP- Duval duct sign
EUS guided pancreatic
biopsy
Whipple’s Pancreato
duodenectomy
Triple bypass
Adjuvant Chemoradio
Peri Ampullary
Carcinoma
Tumors near the
ampulla of Vater
Painless intermittent
jaundice, Silver color
stool, FOBT +ve
CECT and MRI
ERCP- Biopsy
FOBT +ve
Whipple’s Pancreato
Duodenectomy
Adjuvant Chemoradio
Cholangio
Carcinoma
Cancer of the bile ducts
Intra and Extrahepatic
Progressive jaundice
Dark color urine
Pale stools, Itching
CECT and MRI
ERCP
EUS guided FNAC
Surgical resection if
possible
Adjuvant Chemoradio
OBSTRUCTIVE JAUNDICE- Quick Recap












































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)













