Downloaded 81 times


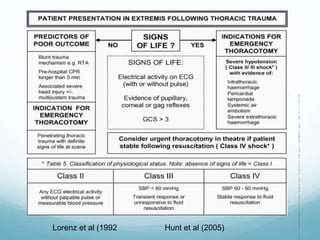
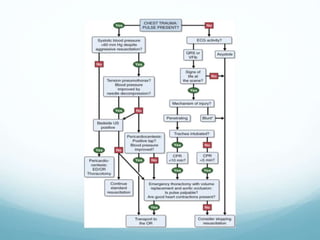






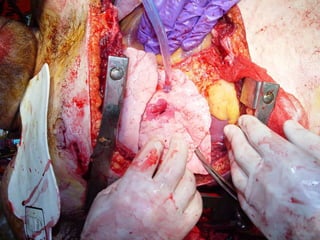


This document discusses emergency thoracotomy procedures for traumatic thoracic injuries. It notes that 25-50% of all traumatic injuries involve the thorax, and that emergency thoracotomy may be necessary for patients experiencing deterioration in the pre-hospital or emergency department setting. The document outlines indications and contraindications for emergency thoracotomy based on whether the injury is penetrating or blunt, lists necessary equipment, describes the procedure steps, and notes factors involved in determining when to terminate the procedure.

































































































