Download as PDF, PPTX






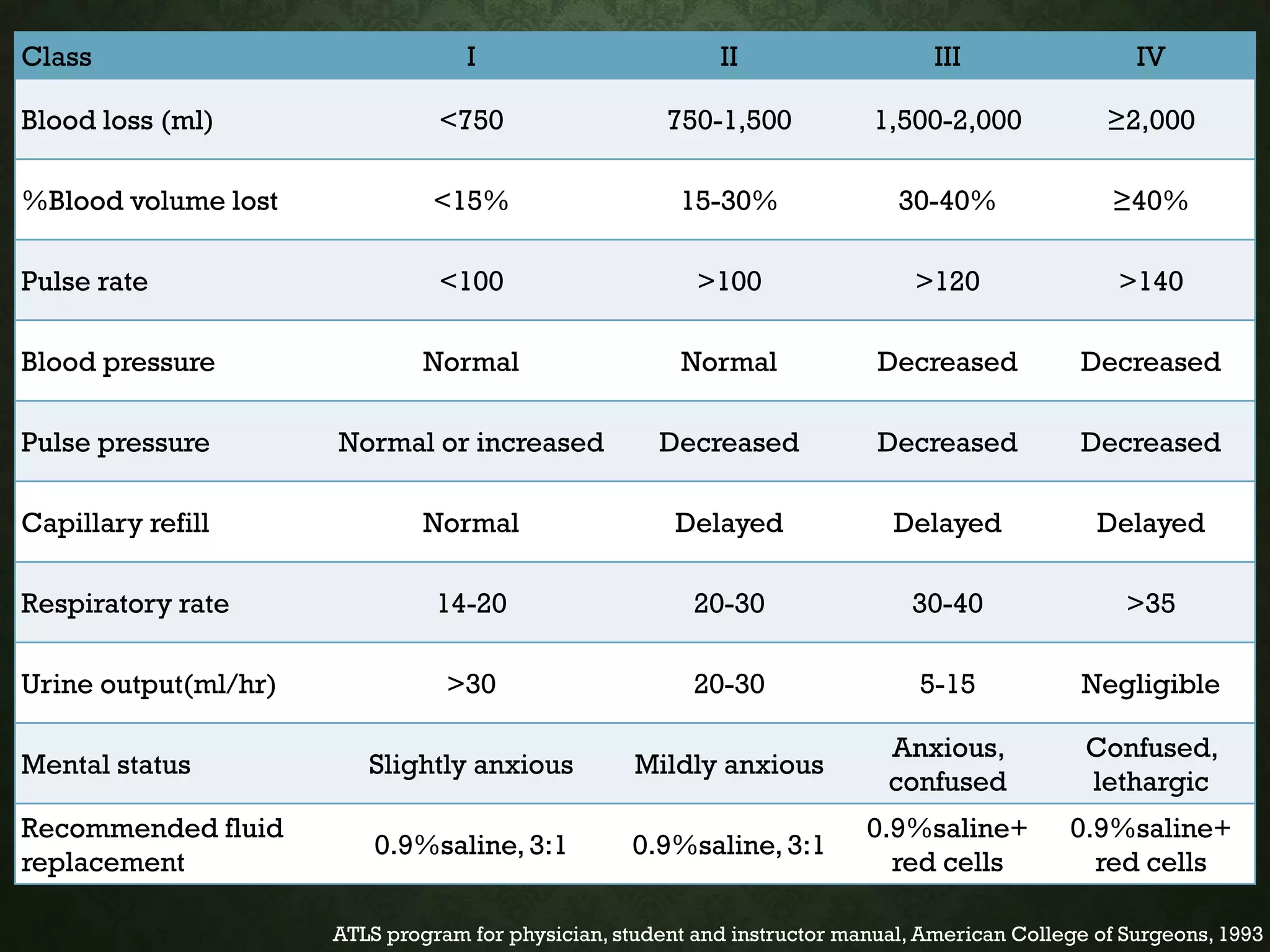

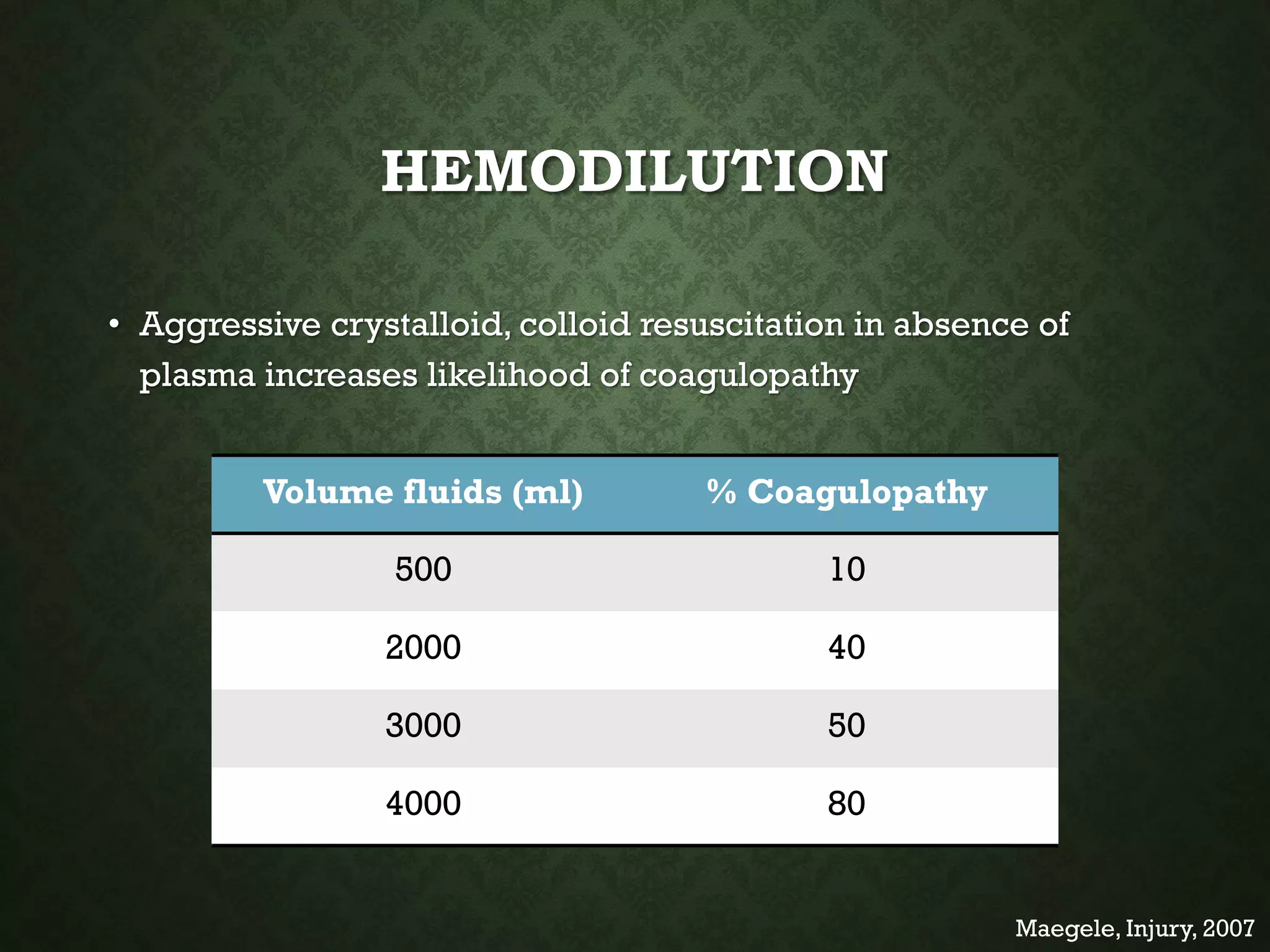








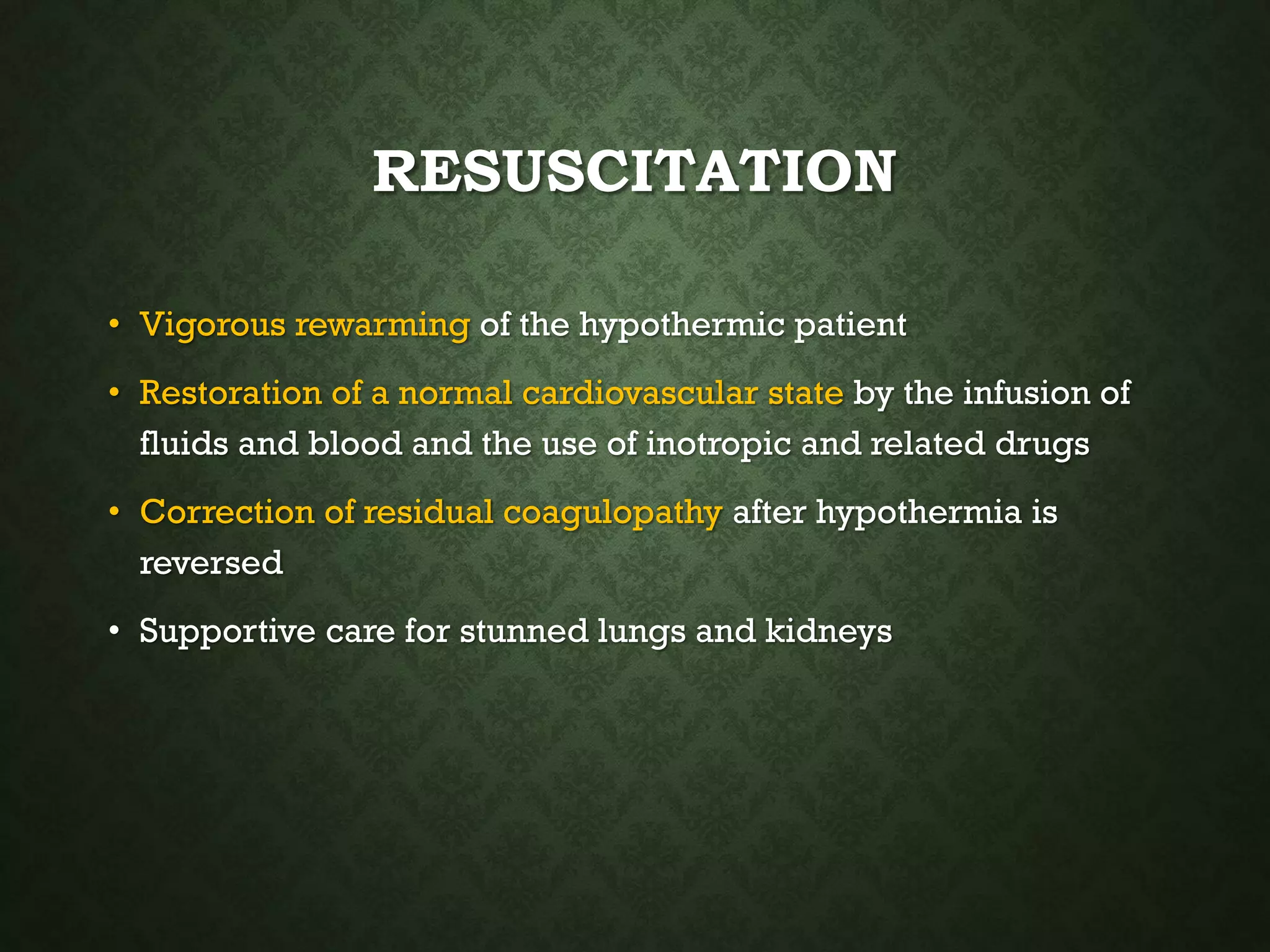


















The document discusses damage control surgery (DCS), which aims to rapidly control hemorrhage and resuscitate patients with profound hemorrhagic shock or metabolic instability. DCS involves limited initial surgery to control bleeding, followed by resuscitation to address hypothermia, acidosis, and coagulopathy ("lethal triad"). The patient then undergoes reoperation once stabilized to complete repairs. Indications for DCS include penetrating thoracic/abdominal wounds with low blood pressure or signs of intra-abdominal bleeding. The goal of resuscitation is to reverse the lethal triad while maintaining permissive hypotension to limit blood loss.























































































