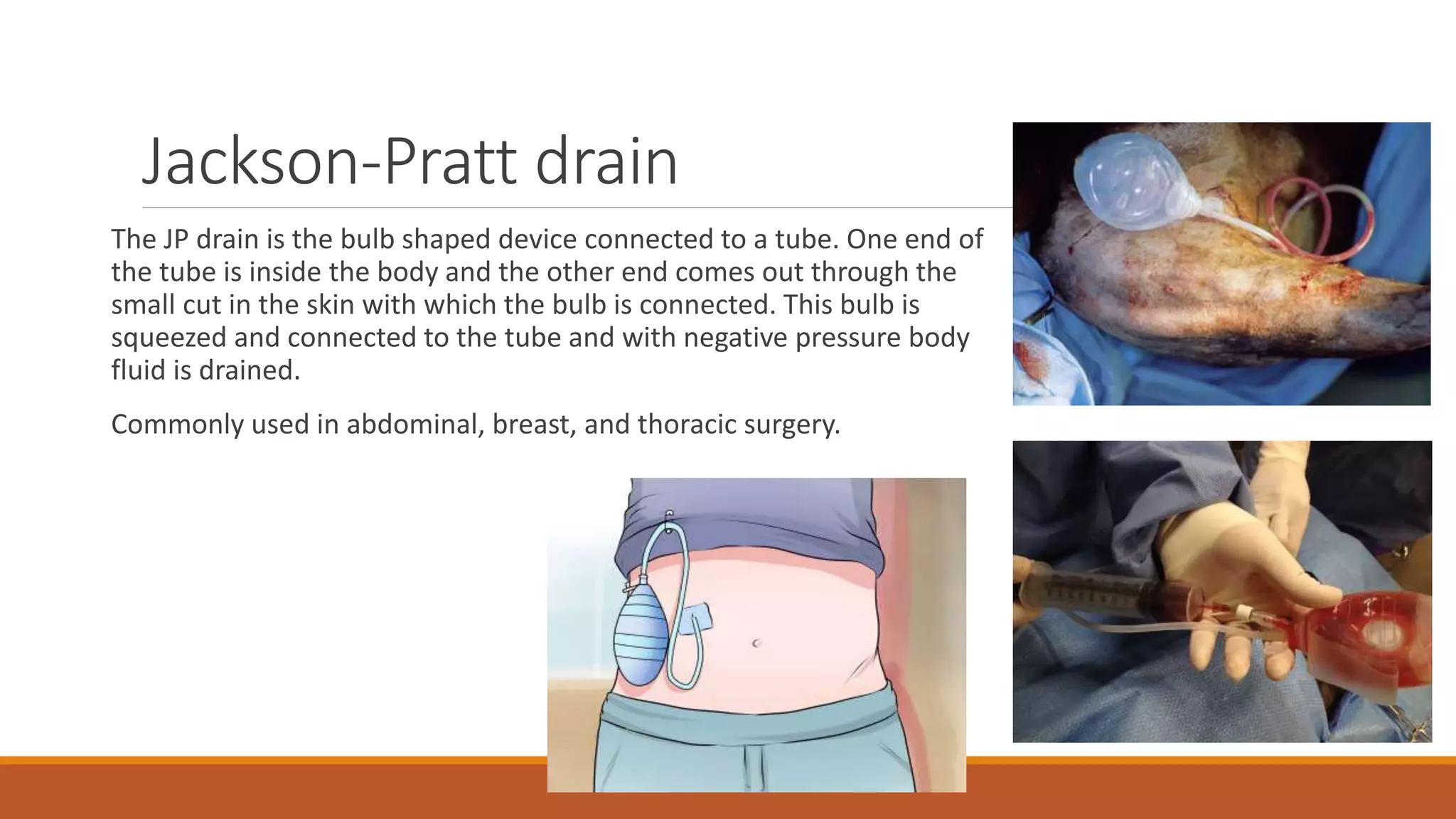
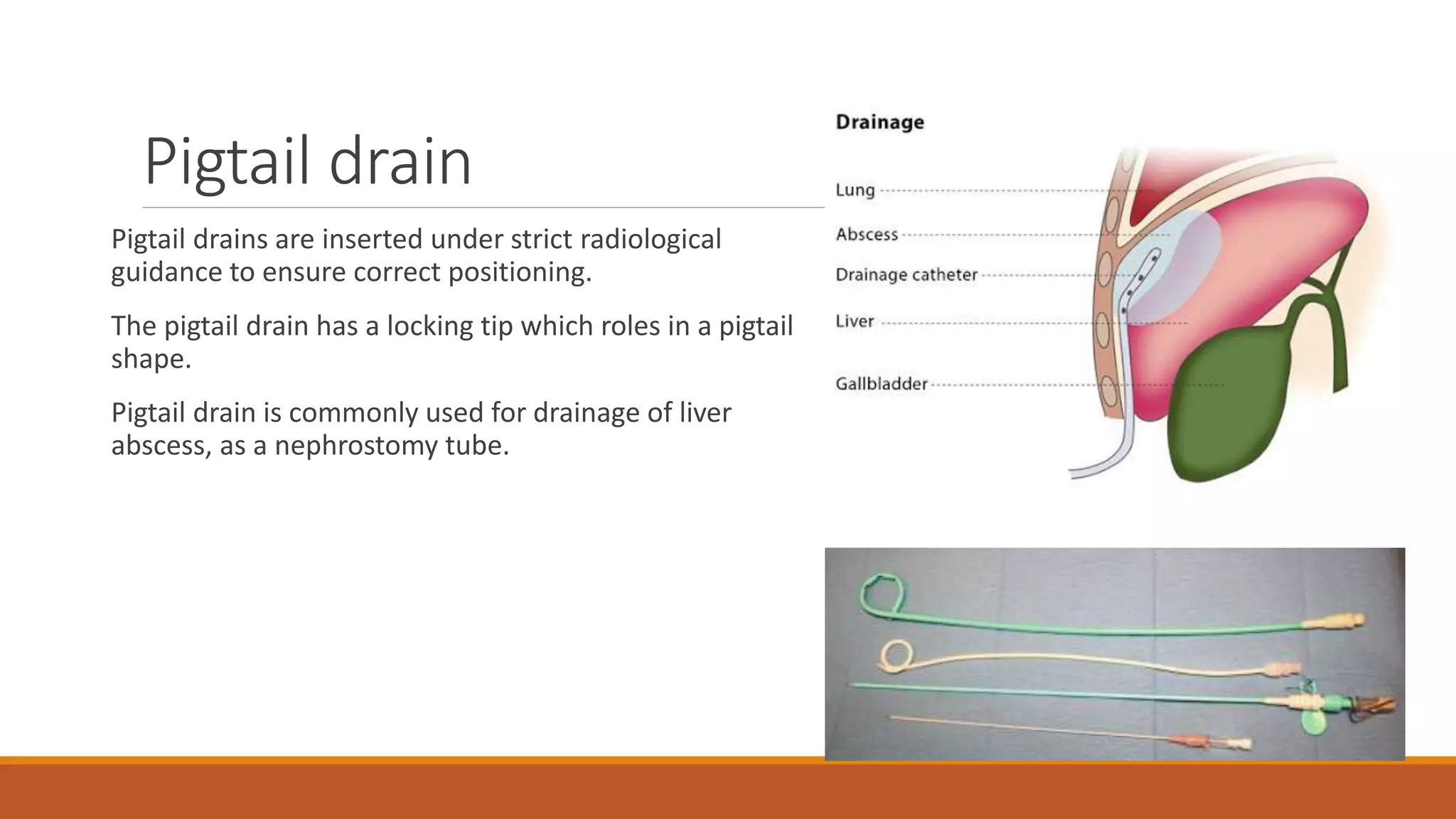
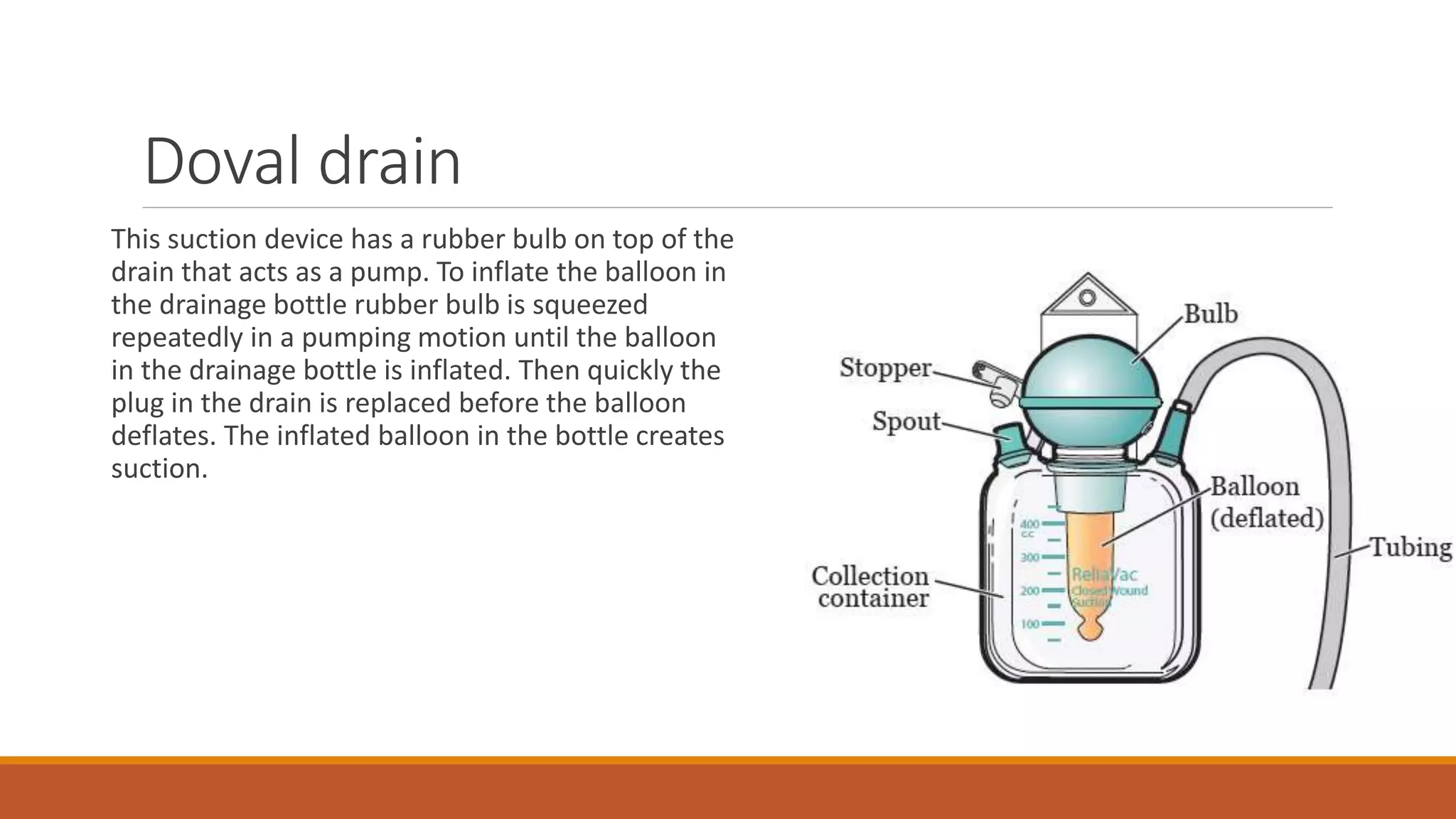
Surgical drains are devices that drain fluids, blood, or air that can accumulate after surgery. There are different types of drains classified as open or closed, and active or passive. Drains are indicated for therapeutic, diagnostic, prophylactic, monitoring, or palliative purposes. Common types include Jackson-Pratt, hemovac, pigtail, and penrose drains. Drains must be properly assessed, maintained if needed, and removed once drainage decreases to prevent complications like infection, blockage, or tissue damage.