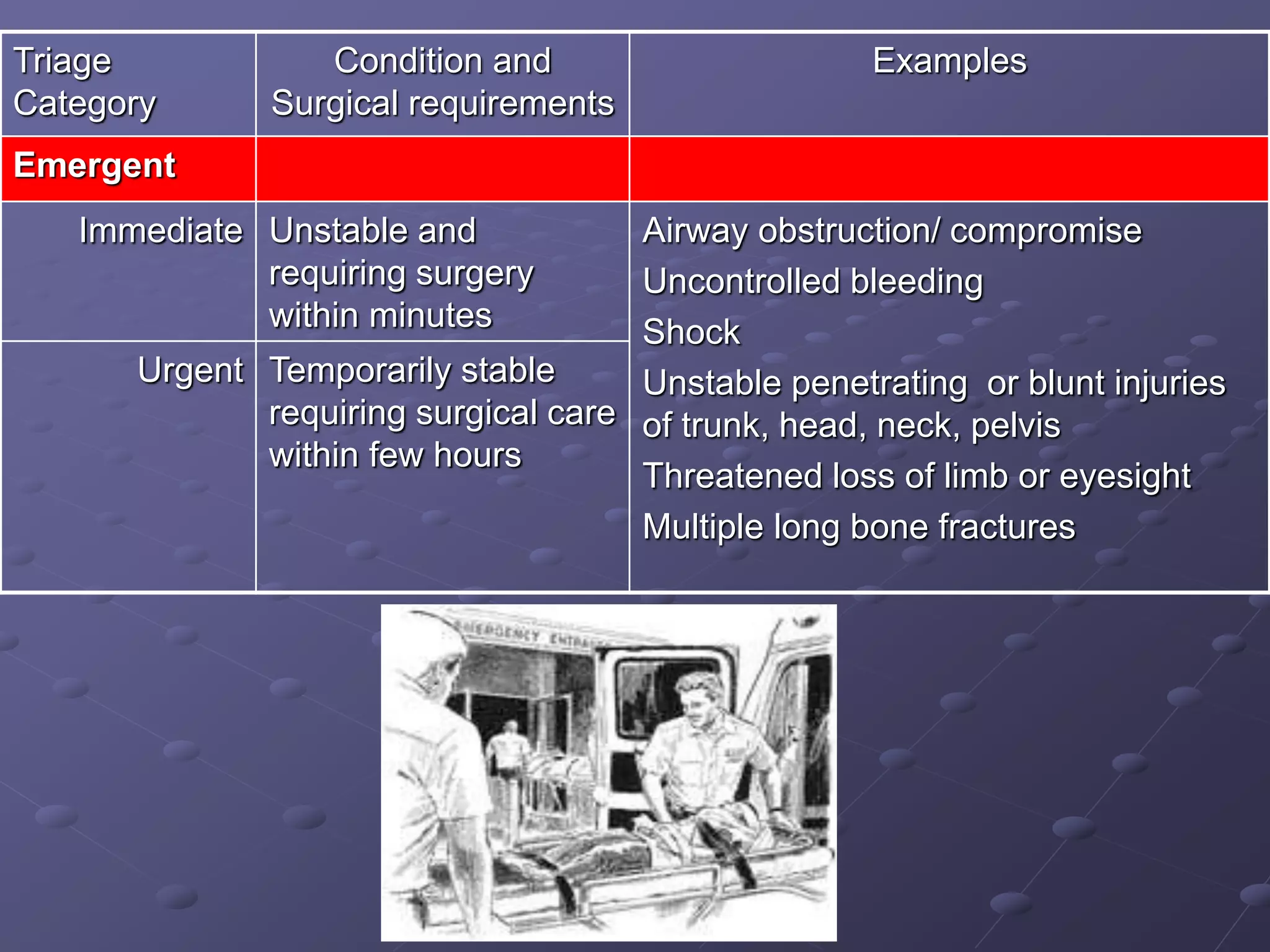
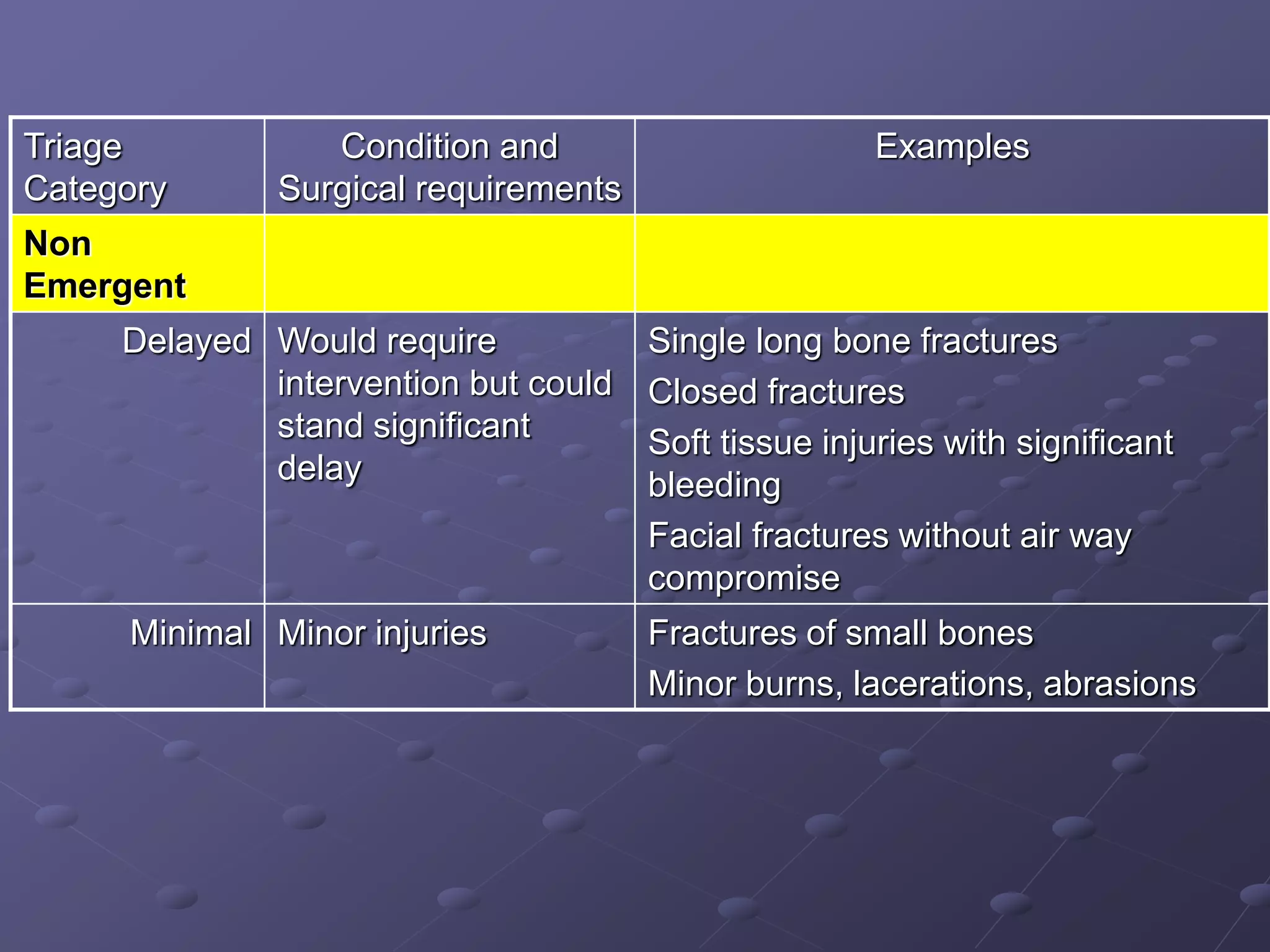
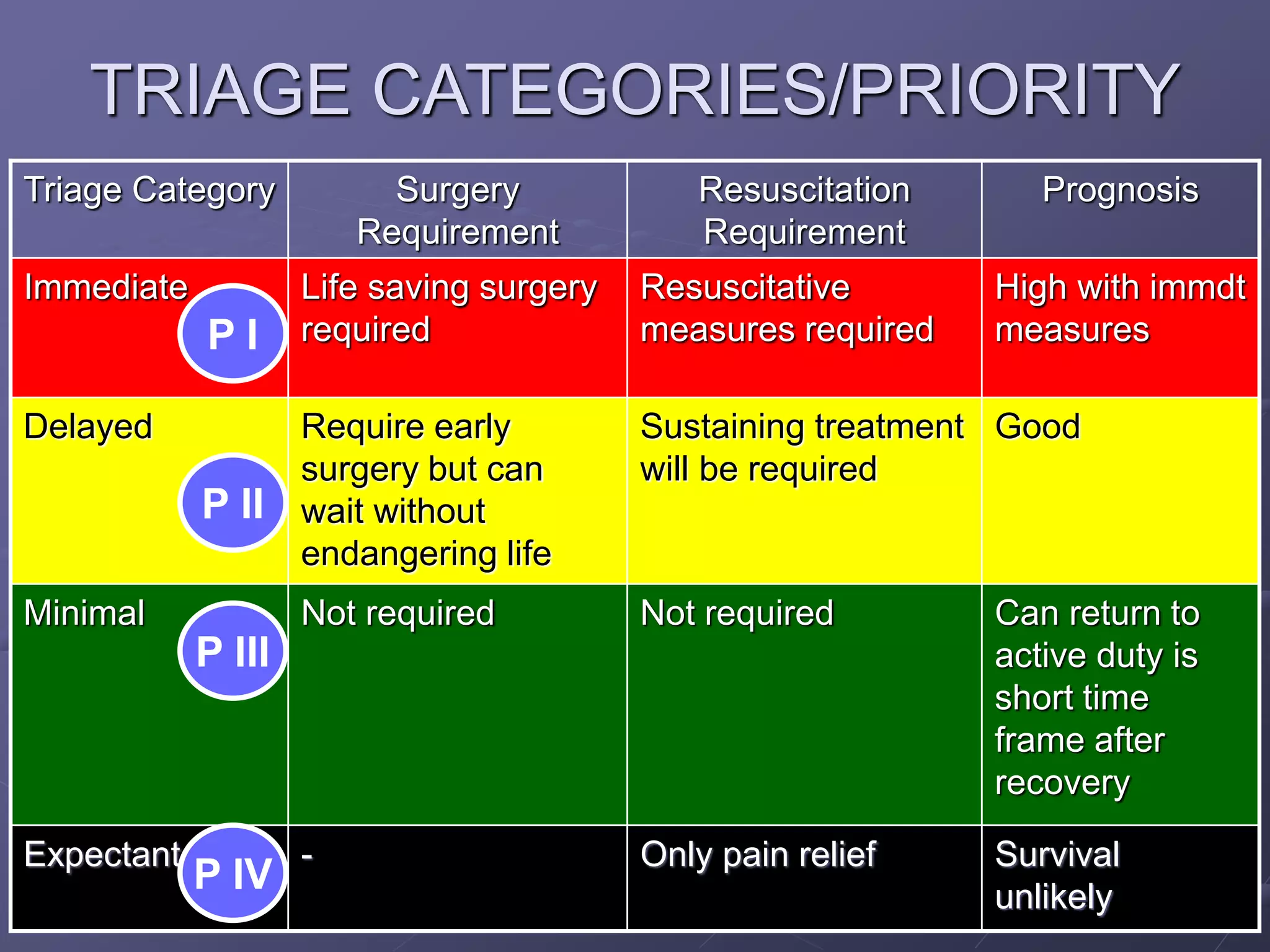
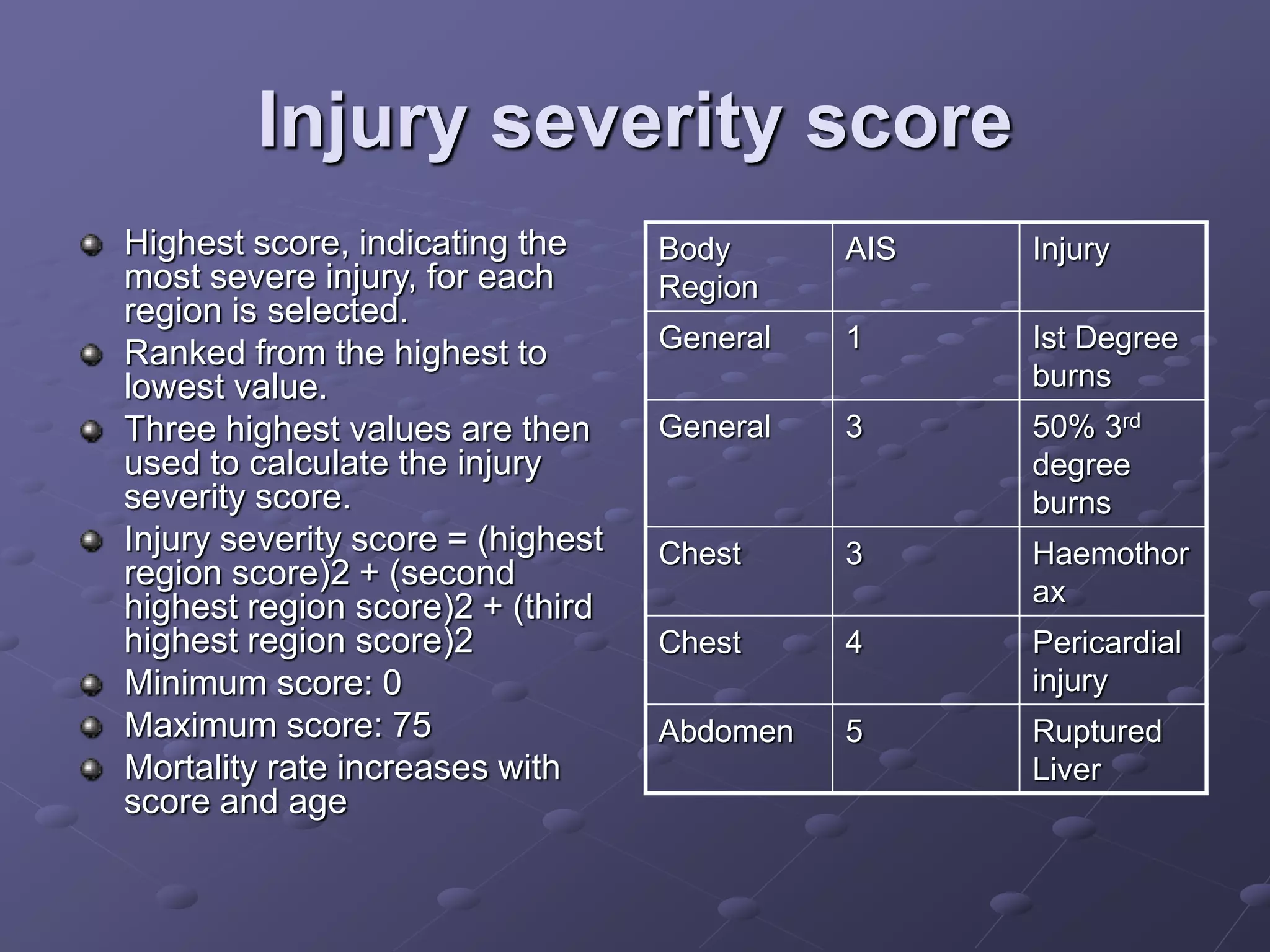
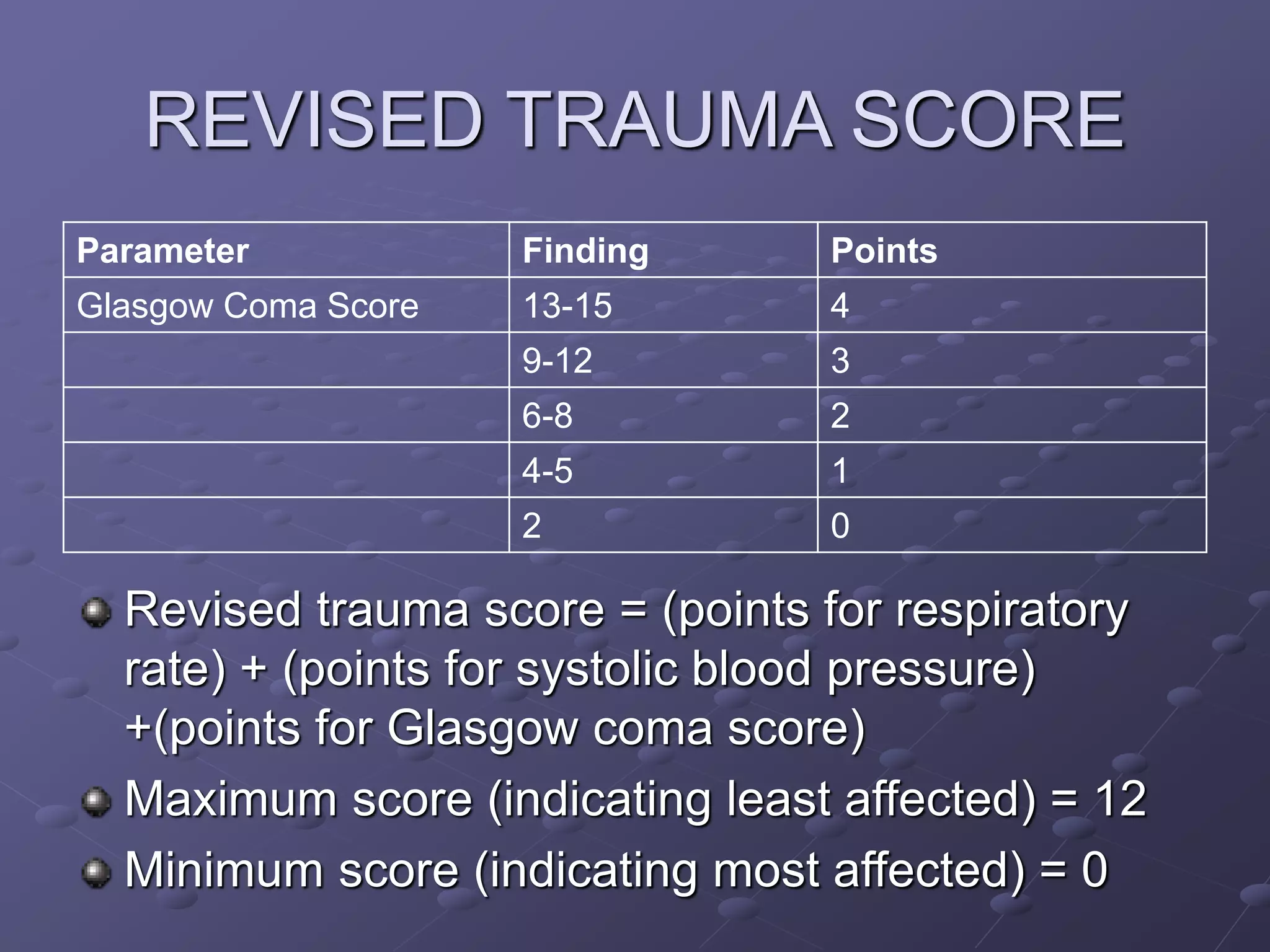
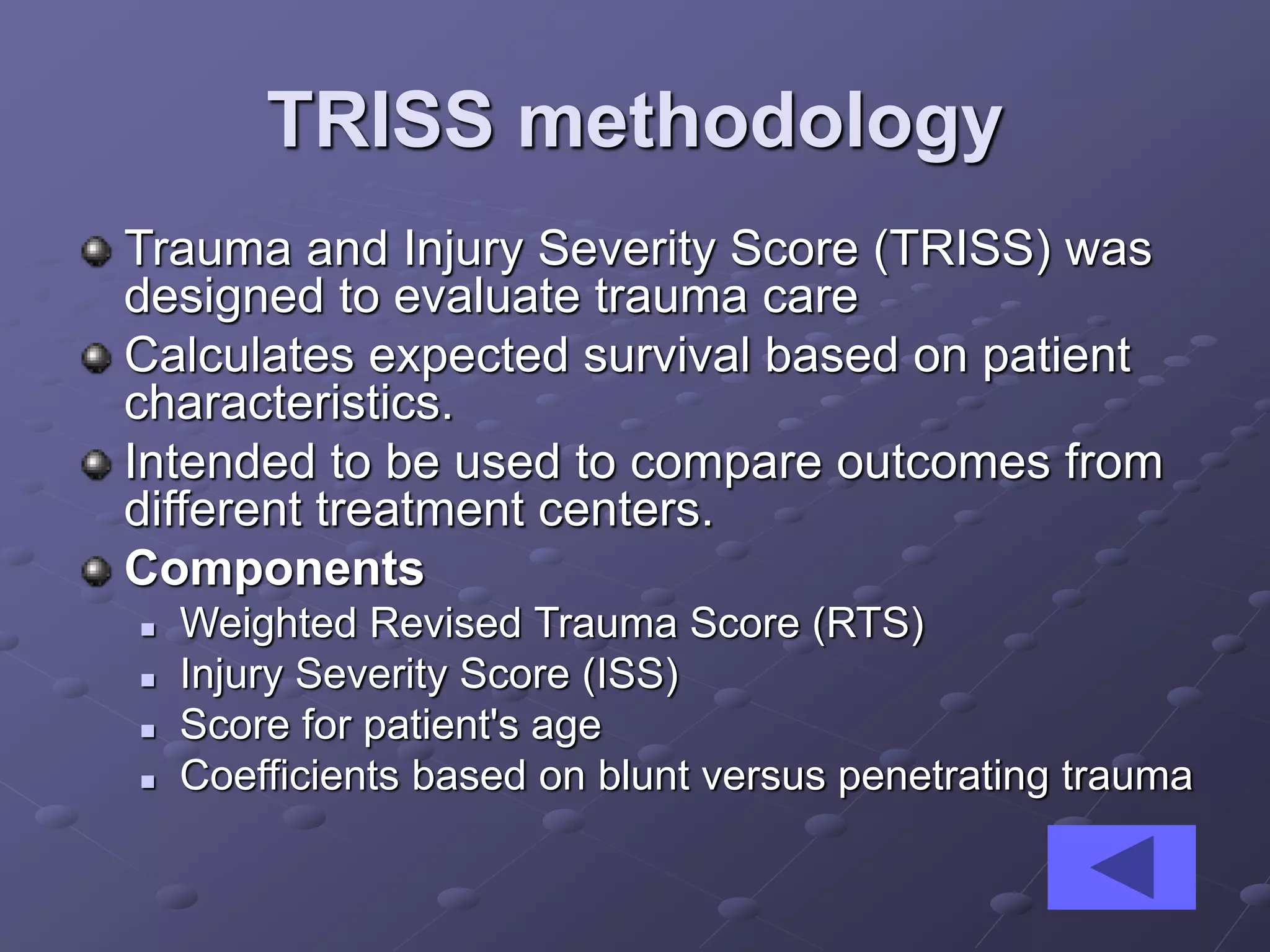
This document discusses methods for triage and assessment in mass casualty situations. It describes evaluating patients based on airway, breathing, circulation, disability and exposure (ATLS methodology). Patients are categorized into triage categories (immediate, delayed, minimal, expectant) based on their injuries and prognosis. Scoring systems like Injury Severity Score (ISS) and Revised Trauma Score (RTS) are used to evaluate patients and compare outcomes between treatment centers using TRISS methodology.