Downloaded 641 times

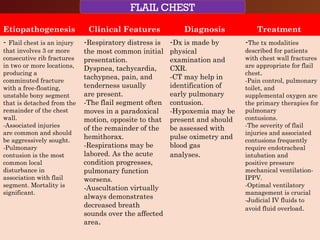
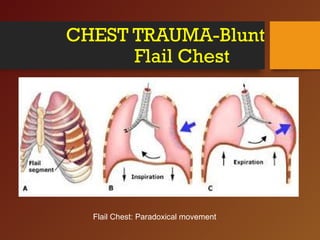
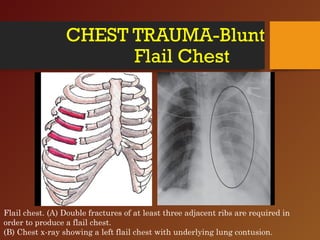
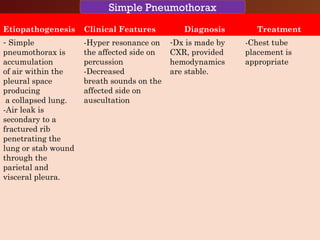
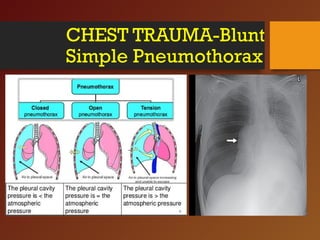
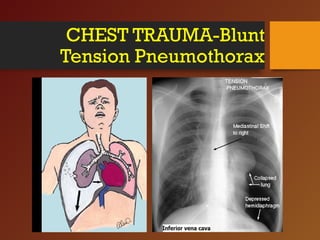


Chest trauma, especially blunt chest trauma, can cause many serious injuries from rib fractures to life-threatening conditions like tension pneumothorax. It is the second leading cause of trauma deaths. Immediate life-threatening injuries include tension pneumothorax, massive hemothorax, flail chest, and cardiac tamponade which must be quickly diagnosed and treated to prevent death. Other potential injuries include pulmonary contusions, pneumothorax, and aortic disruption which require close monitoring and treatment.























































































