Downloaded 143 times
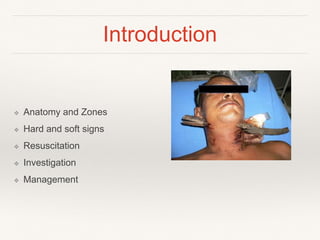

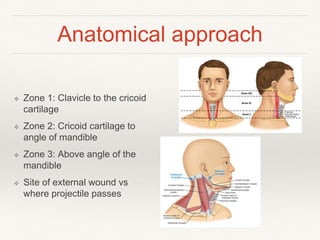
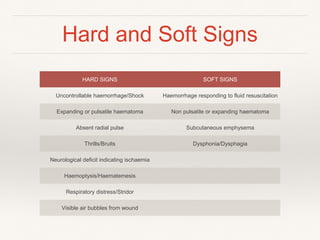

This document discusses penetrating neck trauma. It begins by outlining the anatomy of the neck and dividing it into three zones. It then discusses the mechanisms of injury, signs indicating injury to structures like blood vessels, and considerations for resuscitation and investigation. Hard signs that require emergency surgery include uncontrolled bleeding or shock. Soft signs may allow for further investigation with imaging or endoscopy before deciding on exploration. Surgical management depends on the injured zone, and may involve sternotomy, collar incisions, or mandible resection.






![Penetrating neck trauma [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/penetratingnecktraumaautosaved-191124155903-thumbnail.jpg?width=640&height=640&fit=bounds)
















































































