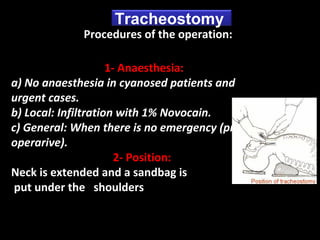
Downloaded 213 times







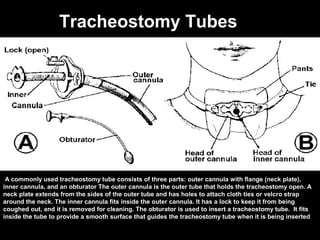
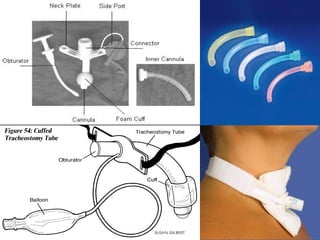












The document discusses tracheostomy, which is a surgical procedure that creates an opening in the windpipe. It has several indications including airway obstruction. A tracheostomy tube consists of an outer cannula, inner cannula, and obturator. Emergency tracheostomies are performed when a person cannot breathe, while nonemergency tracheostomies can be upper, middle, or lower on the trachea. Procedures involve anesthesia, incision, tube insertion, and closing. Complications can be intraoperative like bleeding or late like infection. High risk groups include children, smokers, and the elderly. Postoperative care includes antibiotics and cleaning the tube.






















































































