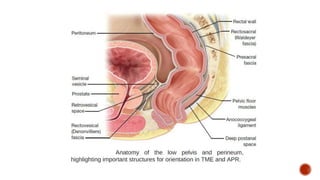
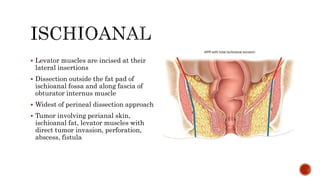
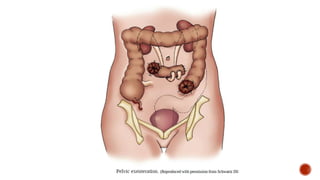
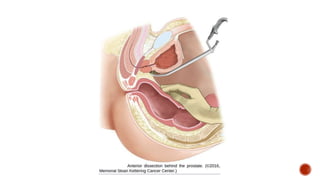
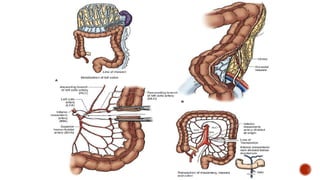
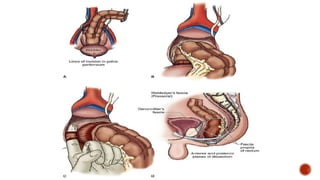
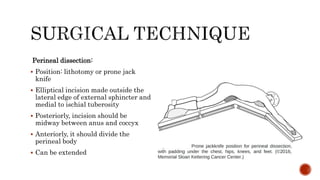
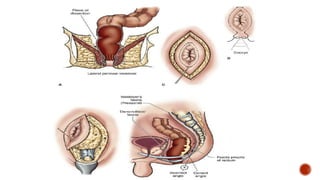
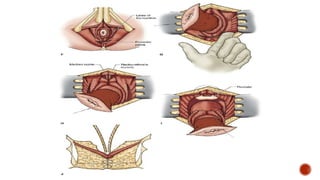
This document discusses the surgical technique for abdominoperineal resection (APR) for rectal cancer. It covers the historical background, indications for APR, preoperative planning including imaging and workup, details of the abdominal and perineal surgical dissections, postoperative care, and management of complications. The key steps of the procedure include a lower abdominal incision to remove the pelvic colon and lymph nodes, followed by an elliptical perineal incision to remove the anus and surrounding tissues while preserving nearby structures like nerves. Postoperative management focuses on early recovery protocols while protecting the perineal wound during healing. Common complications include perineal wound issues and genitourinary dysfunction.