Downloaded 202 times






















![CSF Immunoglobulin
CSF IgG/Serum IgG
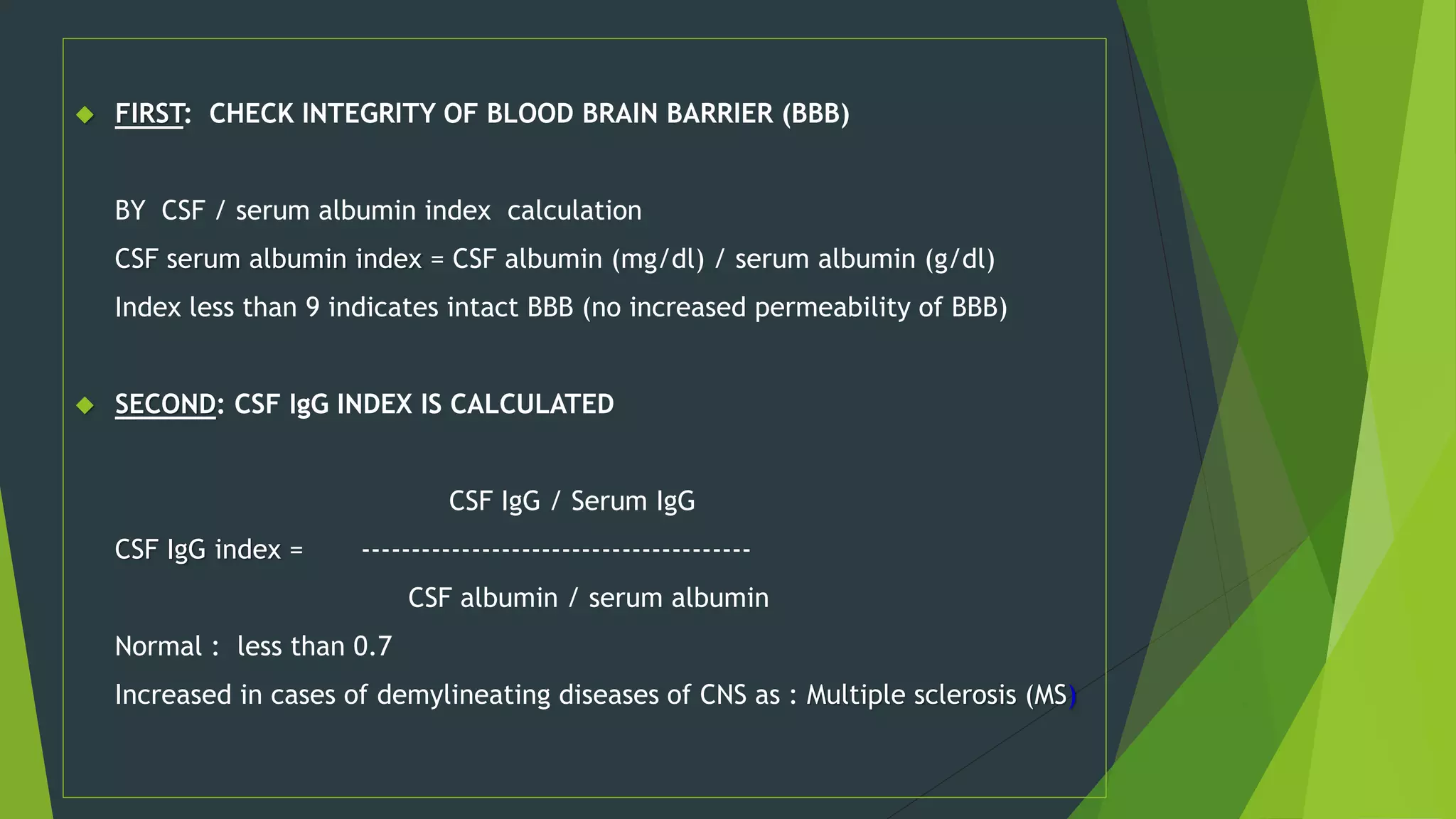
CSF serum /Albumin index
CSF IgG can arise:
1)from plasma cells within CSF
2) from the blood through BBB
CSF IgG index:
Normally: < 0.7
=
↑CSF [IgG] without concomitant ↑ in CSF [Alb] suggests local
production of IgG:
multiple sclerosis (MS)
subacute sclerosing panencephalitis (SPEE)](https://image.slidesharecdn.com/anveshcerebrospinalfluidanalysis-141014225425-conversion-gate02/75/cerebro-spinal-fluid-analysis-27-2048.jpg)




![Other Chemical Components of
CSF
CSF [Calcium], [Potassium] & [Phosphates] are lower
than their levels in the blood
CSF [Chloride] & [Magnesium] are higher than their
levels in the blood
Abnormal CSF [Chloride]
marked in acute bacterial meningitis
slight in viral meningitis & brain tumors](https://image.slidesharecdn.com/anveshcerebrospinalfluidanalysis-141014225425-conversion-gate02/75/cerebro-spinal-fluid-analysis-32-2048.jpg)



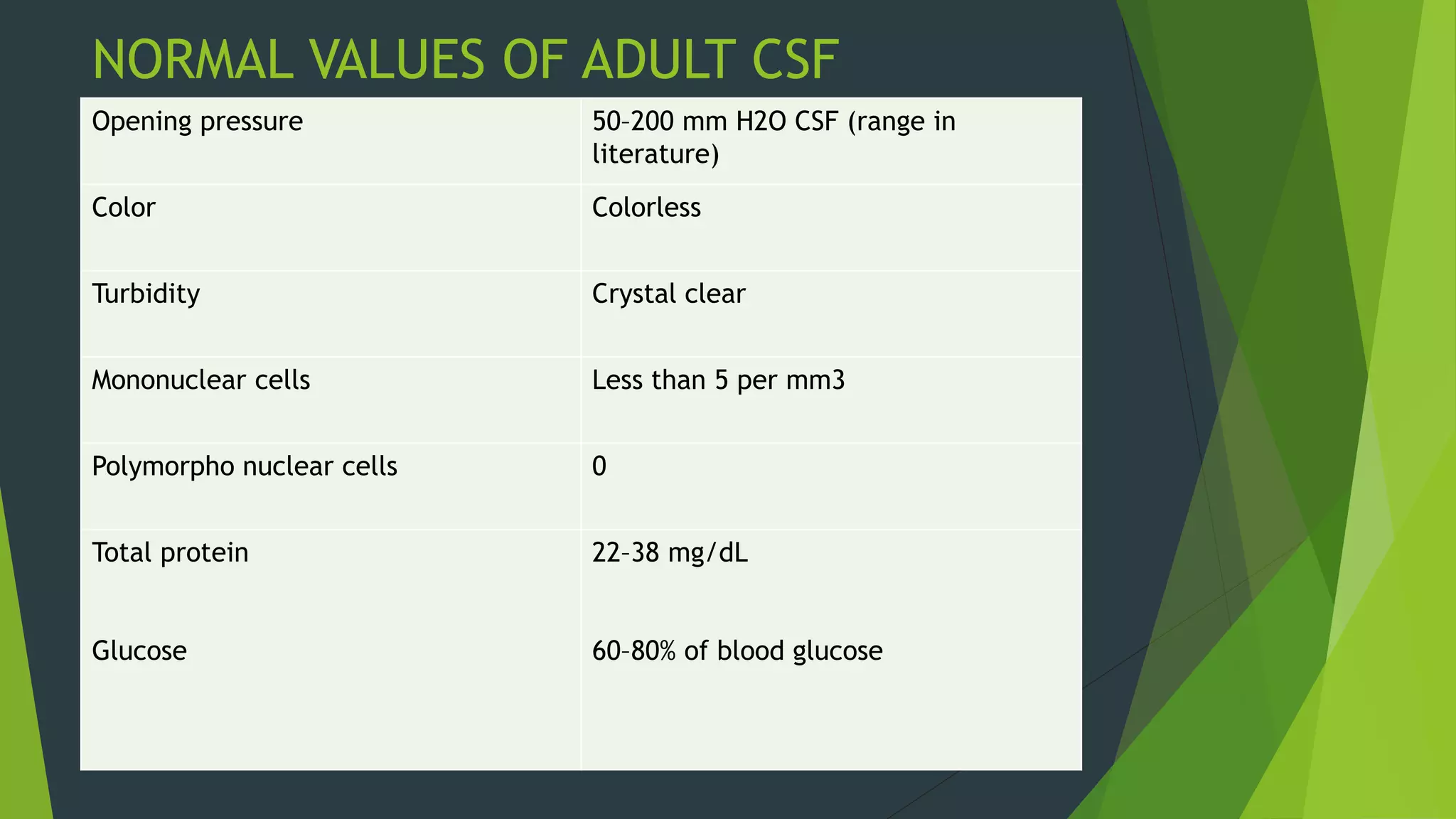
The document provides information on cerebrospinal fluid (CSF) analysis, including its production, circulation, and examination. It discusses normal CSF values and abnormalities seen in various conditions. The lumbar puncture procedure and complications are also outlined. Abnormalities in CSF parameters like increased white blood cells, decreased glucose, and elevated proteins can indicate infections like bacterial meningitis, while more subtle changes may be seen in viral meningitis and tuberculosis meningitis. CSF analysis is useful for diagnosis.











































































































