Downloaded 505 times


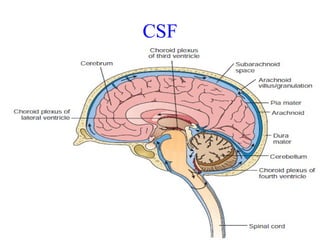
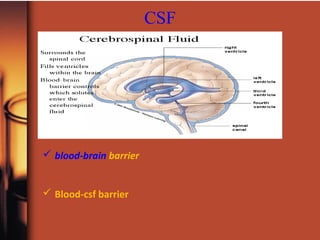
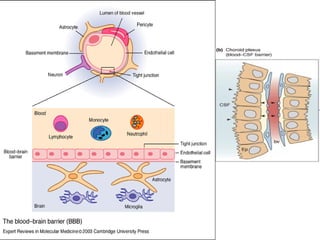

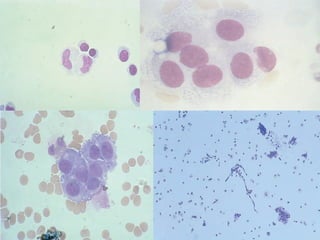
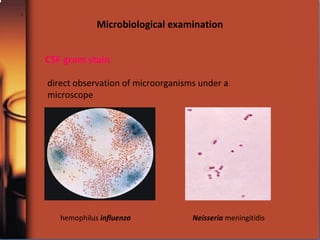


Cerebrospinal fluid (CSF) provides nutrients and removes waste from the central nervous system. CSF analysis can help diagnose diseases affecting the brain and spinal cord like infections, bleeding, tumors, and inflammation. CSF is collected via lumbar puncture and analyzed through various tests. Microscopic examination identifies cell types which can indicate conditions, and microbiological tests can identify infectious organisms. Overall, CSF analysis is a valuable tool for evaluating central nervous system diseases.
























































![CSF CNS covered by 3 membranes [meninges] pdf](https://cdn.slidesharecdn.com/ss_thumbnails/csf-240227110022-60ed50a9-thumbnail.jpg?width=640&height=640&fit=bounds)






























