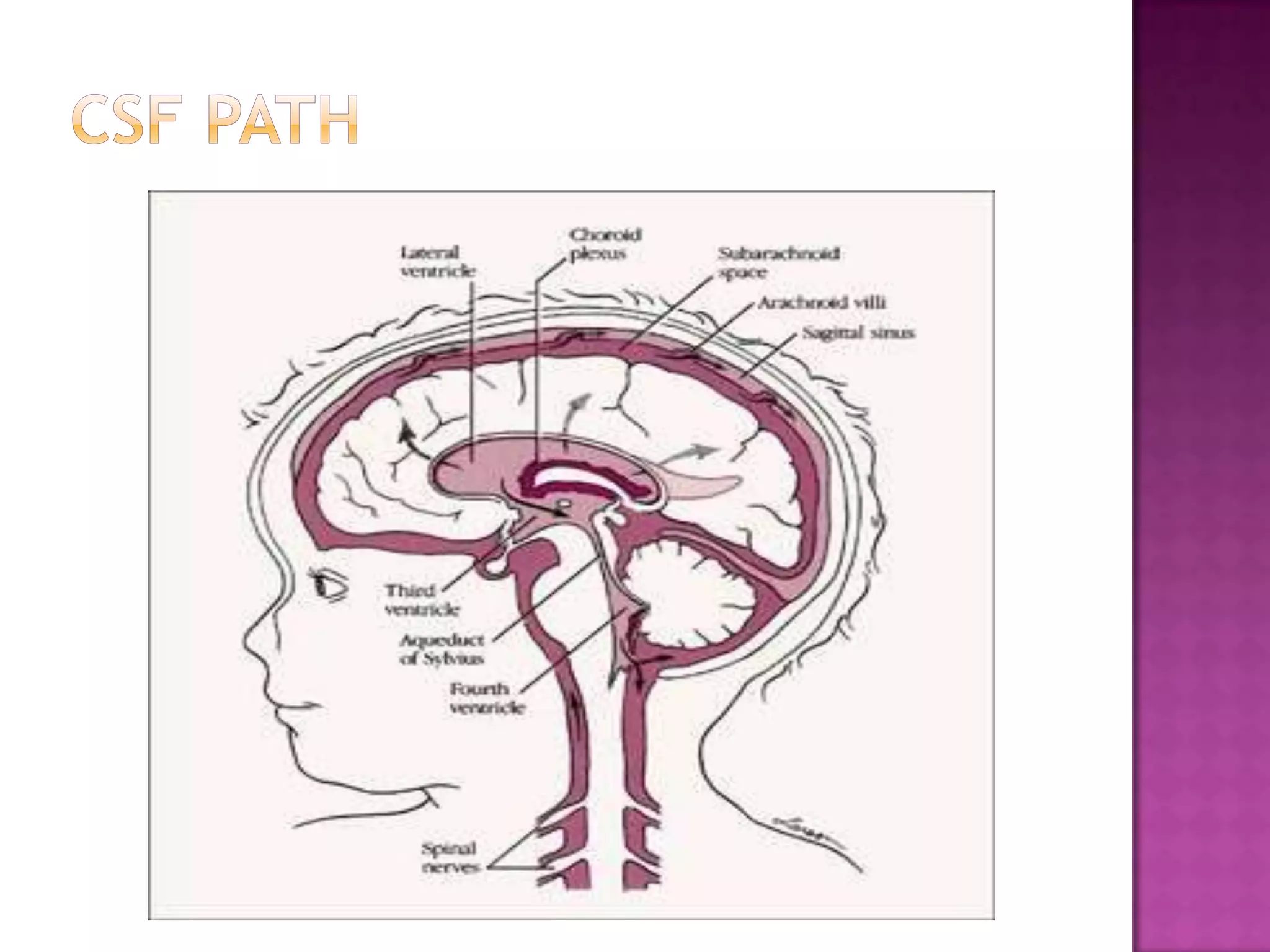
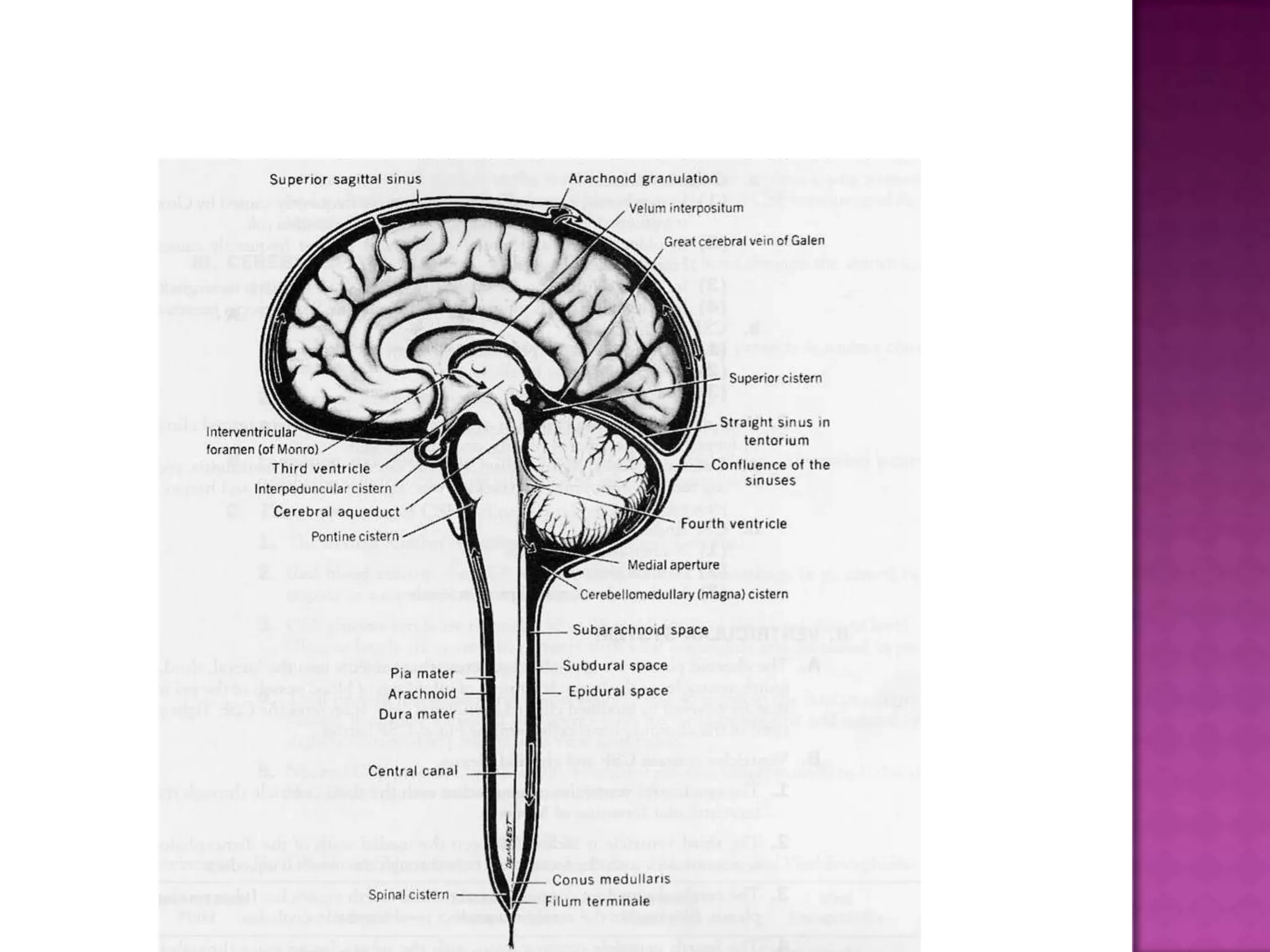
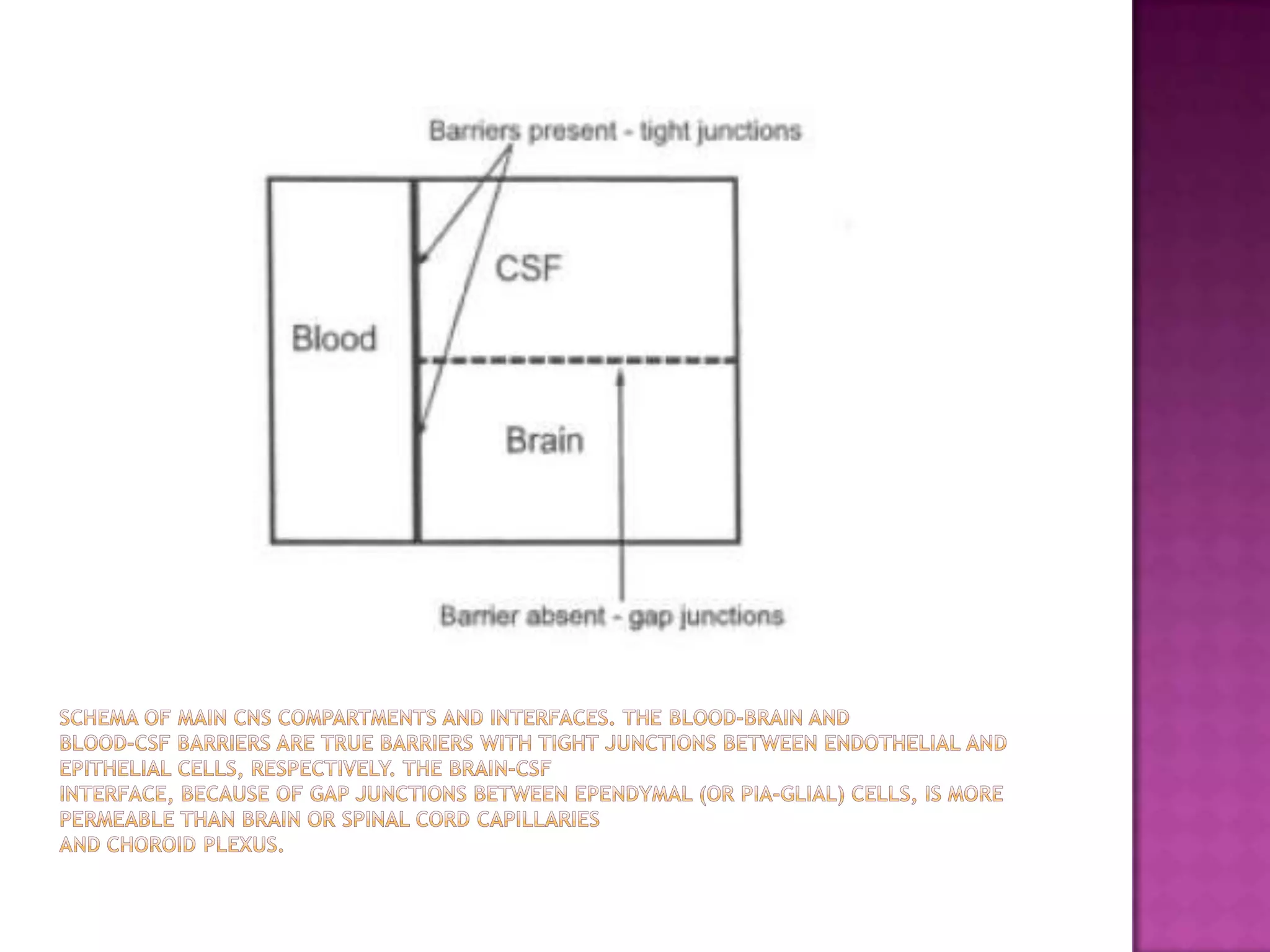
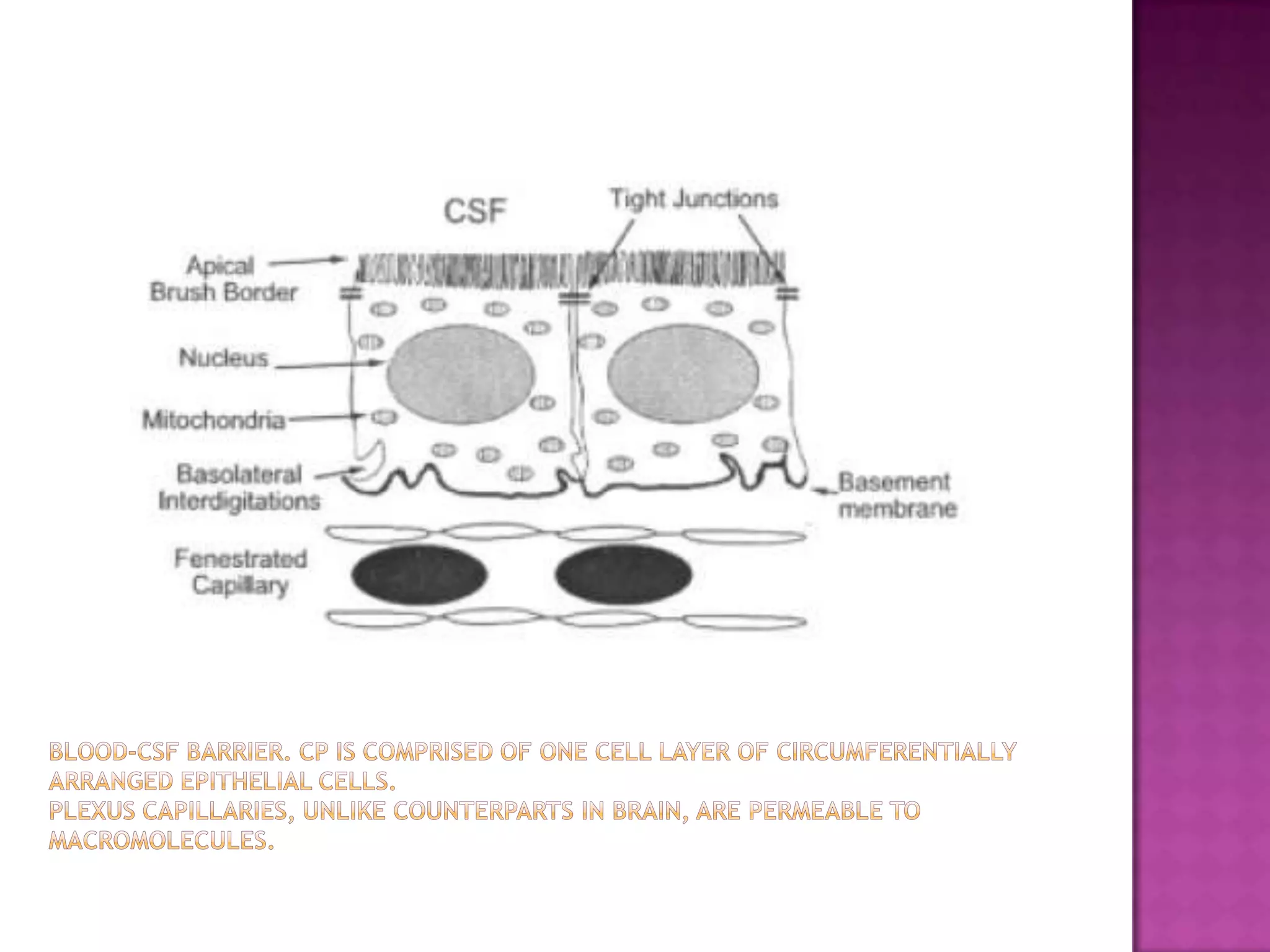
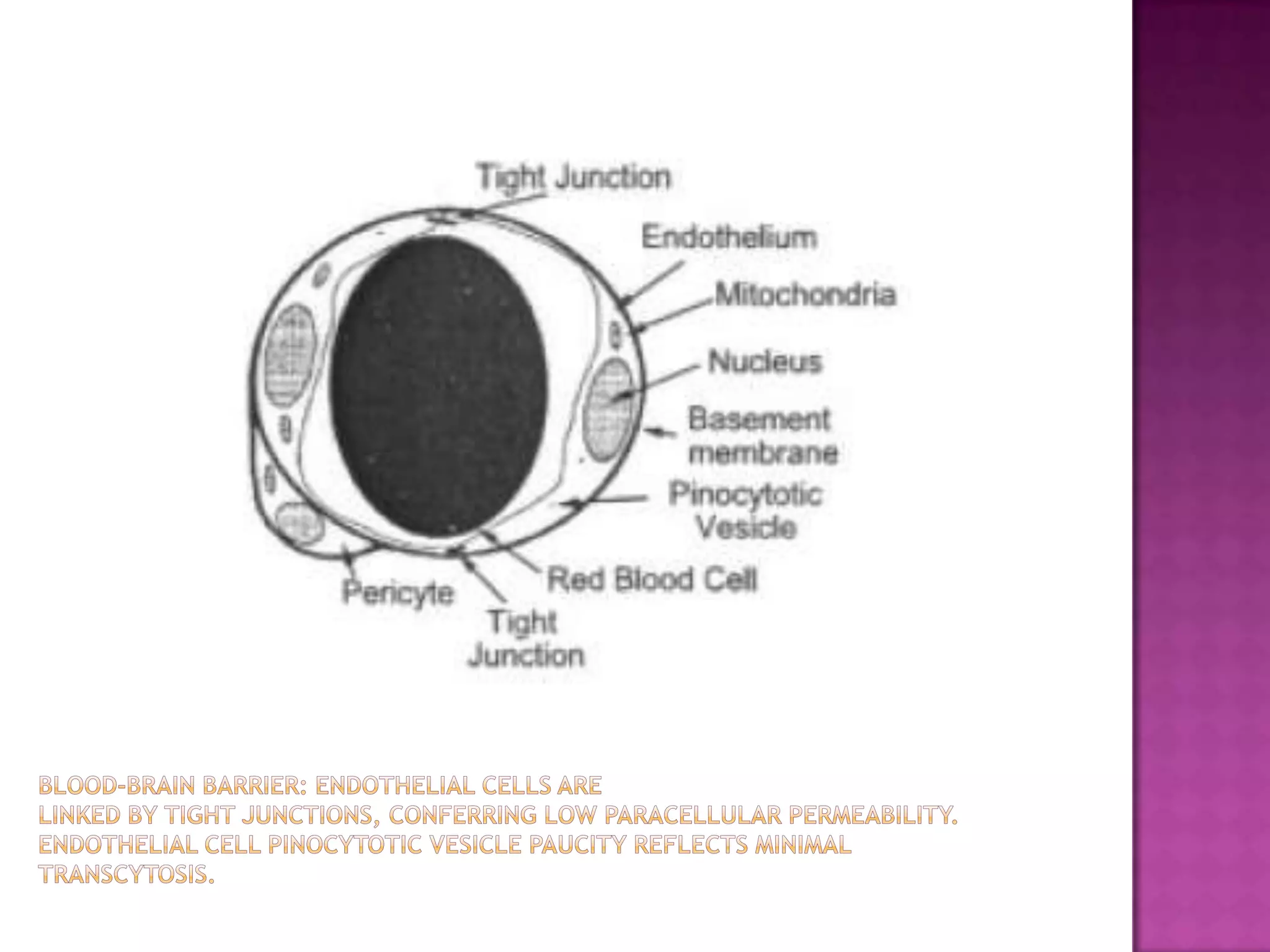
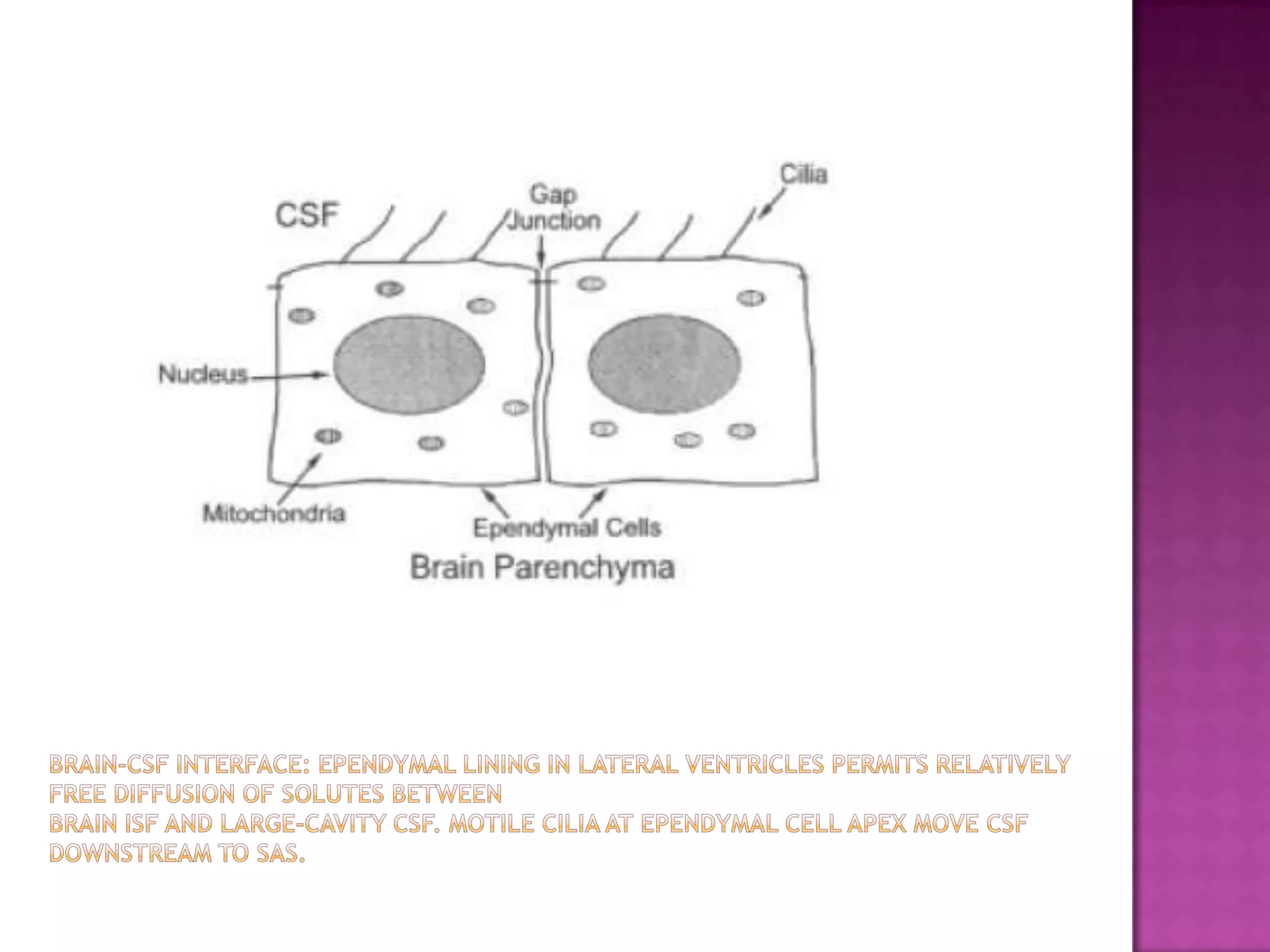


The document discusses cerebrospinal fluid (CSF), including its production and pathways in the central nervous system. CSF acts as a cushion or buffer for the brain, is produced by the choroid plexus at a rate of around 500 ml per day, and circulates through the ventricular system and subarachnoid space. Analysis of CSF provides valuable information for diagnosing neurological conditions through examination of cells, proteins, glucose, and other analytes. Abnormal levels can indicate infections, inflammatory conditions, and other disorders.








































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)














