Downloaded 1,116 times
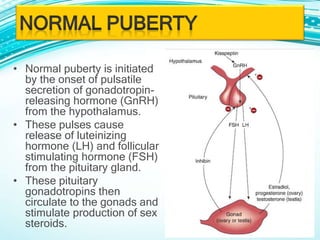
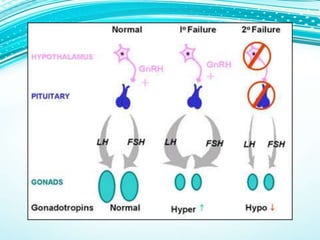


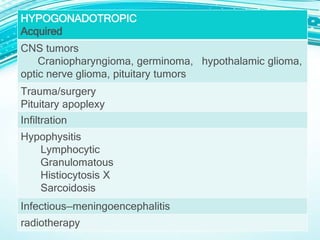
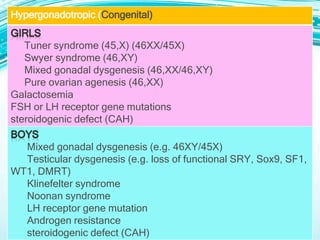



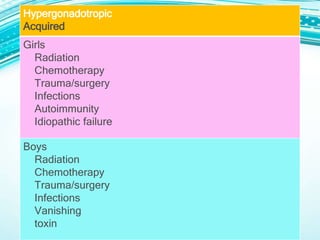
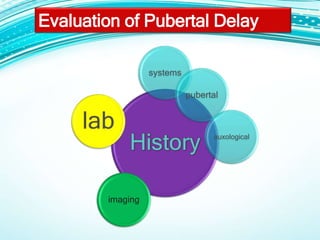


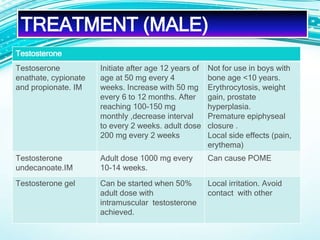
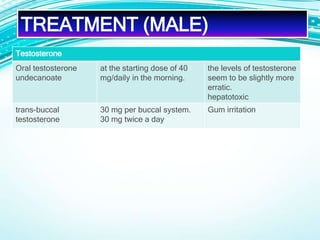

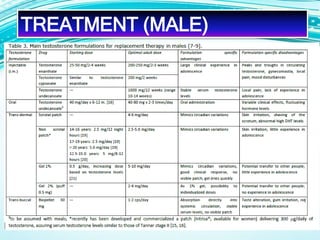
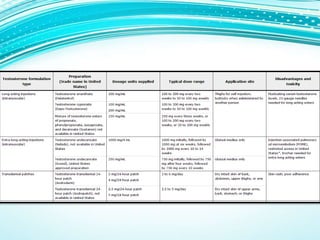
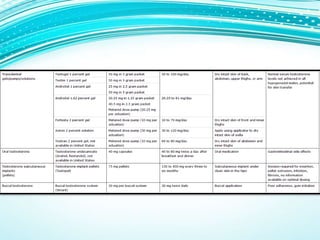




This document provides information on evaluating and treating delayed puberty. It defines delayed puberty and discusses the main causes, which include constitutional delay of puberty, hypogonadotropic hypogonadism, and hypergonadotropic hypogonadism. Evaluation involves assessing medical history, physical exam including Tanner staging, lab tests of hormone levels, bone age, and imaging if needed. Treatment depends on the underlying cause, and may include observation, sex hormone therapy, or treating any underlying medical conditions.


































































![APPLIED ASPECTS OF PUBERTY AND ADOLESCENCE (final)[1].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/appliedaspectsofpubertyandadolescencefinal1-250718083958-0c4146c6-thumbnail.jpg?width=640&height=640&fit=bounds)








































