Downloaded 56 times
![BBB:
• The tight junctions between the epithelial cells of the
capillaries and those of the choroid plexus form the
blood-brain barrier:
– prevents the free movement of large and/or hydrophilic
molecules from plasma to CSF and
– facilitates movement of essential molecules like glucose (via
GLUT 1 transporter) into the CSF.
• Fat soluble molecules cross easily, as do O2 and CO2 .
• In contrast HCO3- and H+ do not cross easily and rely
on Carbonic Anhydrase in the choroid plexus to
regenerate them from CO2 & H2O, the [H+] in CSF
being essential in regulating respiration.](https://image.slidesharecdn.com/csfinclinico-laboratorydiagnoses-191004112029/75/Csf-in-clinico-laboratory-diagnoses-4-2048.jpg)
![Chemistry of normal CSF vs plasma
CSF Plasma CSF/Plasma %
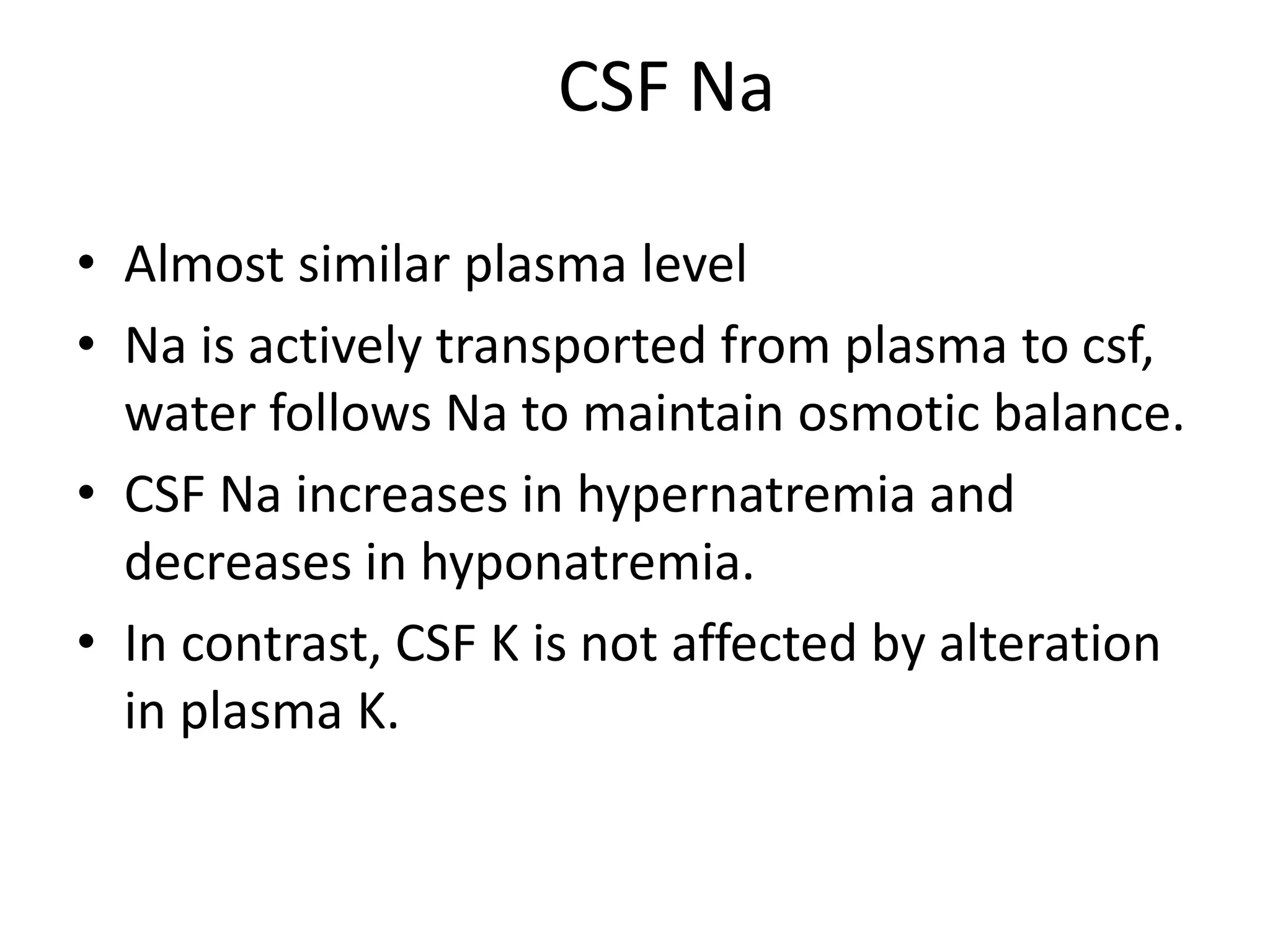
• Na (mmol/l) 140 140 100
• K (mmol/l) 3 4.5 65%
• Cl (mmol/l) 118 99 114%
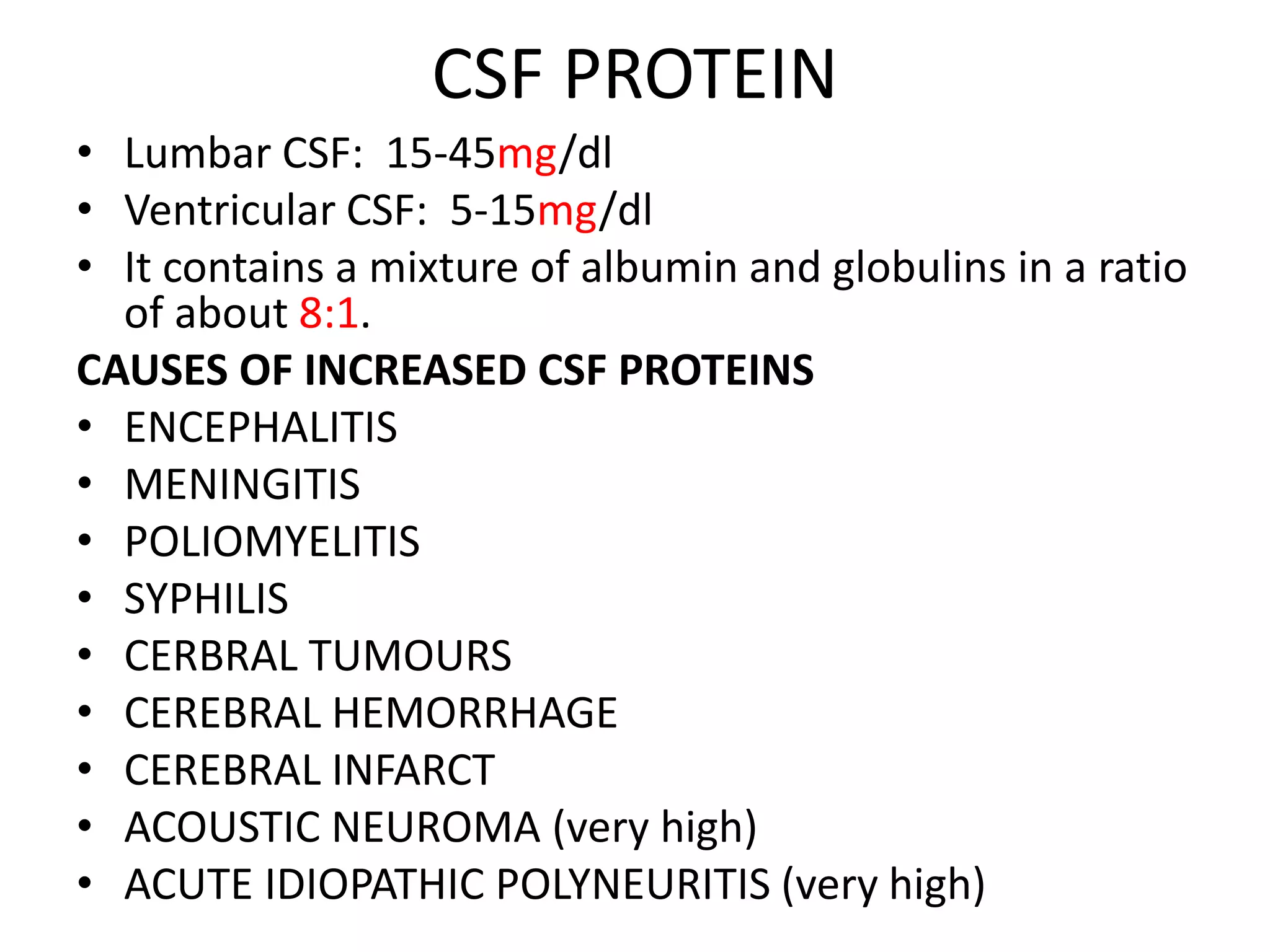
• Protein (g/l) 0.2 60 0.3% (CSF is 1/200 of serum)
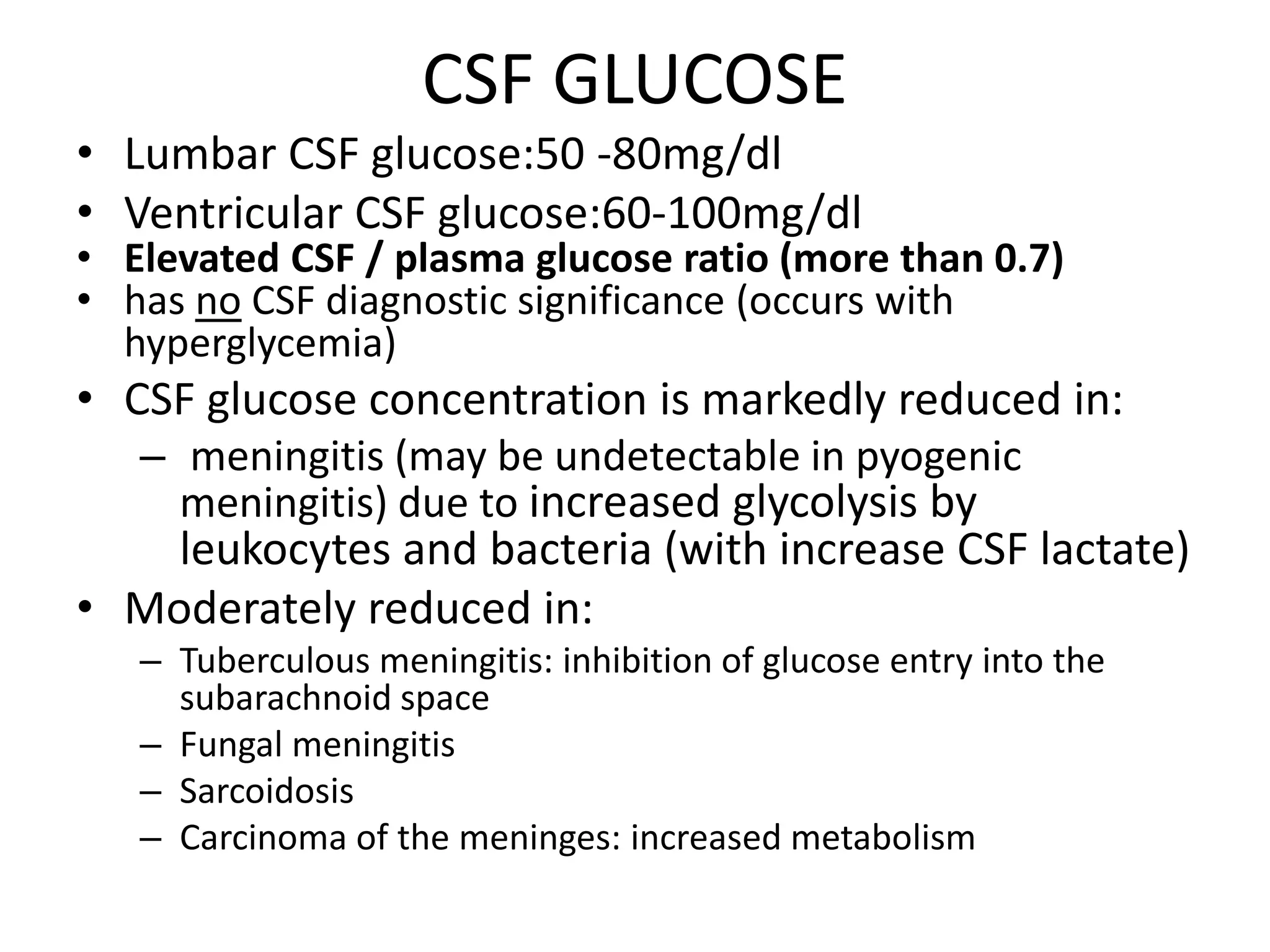
• Glu(mmol/L) 3 5 60% (2/3 of plasma)
• CSF [Calcium], [Potassium] & [Phosphates] are lower than their levels in
the blood
• CSF [Chloride] & [Magnesium] are higher than their levels in the blood
OTHERS:
• BICARBONATE: 23.6MMOL/L
• IMMUOGLOBULINS: IgG,A,M
• PRESSURE: 80-180mmH2O
• R.B.C: 0
• W.B.C: Total w.b.c count<5
Neutrophils 0-1](https://image.slidesharecdn.com/csfinclinico-laboratorydiagnoses-191004112029/75/Csf-in-clinico-laboratory-diagnoses-5-2048.jpg)
![OTHER CHEMICAL COMPONENTS:
• Lactate levels are used mostly to distinguish early
bacterial meningitis from viral meningitis.
• LD activity is significantly higher in bacterial
meningitis than in aseptic meningitis.
• CSF [Calcium], [Potassium] & [Phosphates] are
lower than their levels in the blood
• CSF [Chloride] & [Magnesium] are higher than
their levels in the blood](https://image.slidesharecdn.com/csfinclinico-laboratorydiagnoses-191004112029/75/Csf-in-clinico-laboratory-diagnoses-17-2048.jpg)
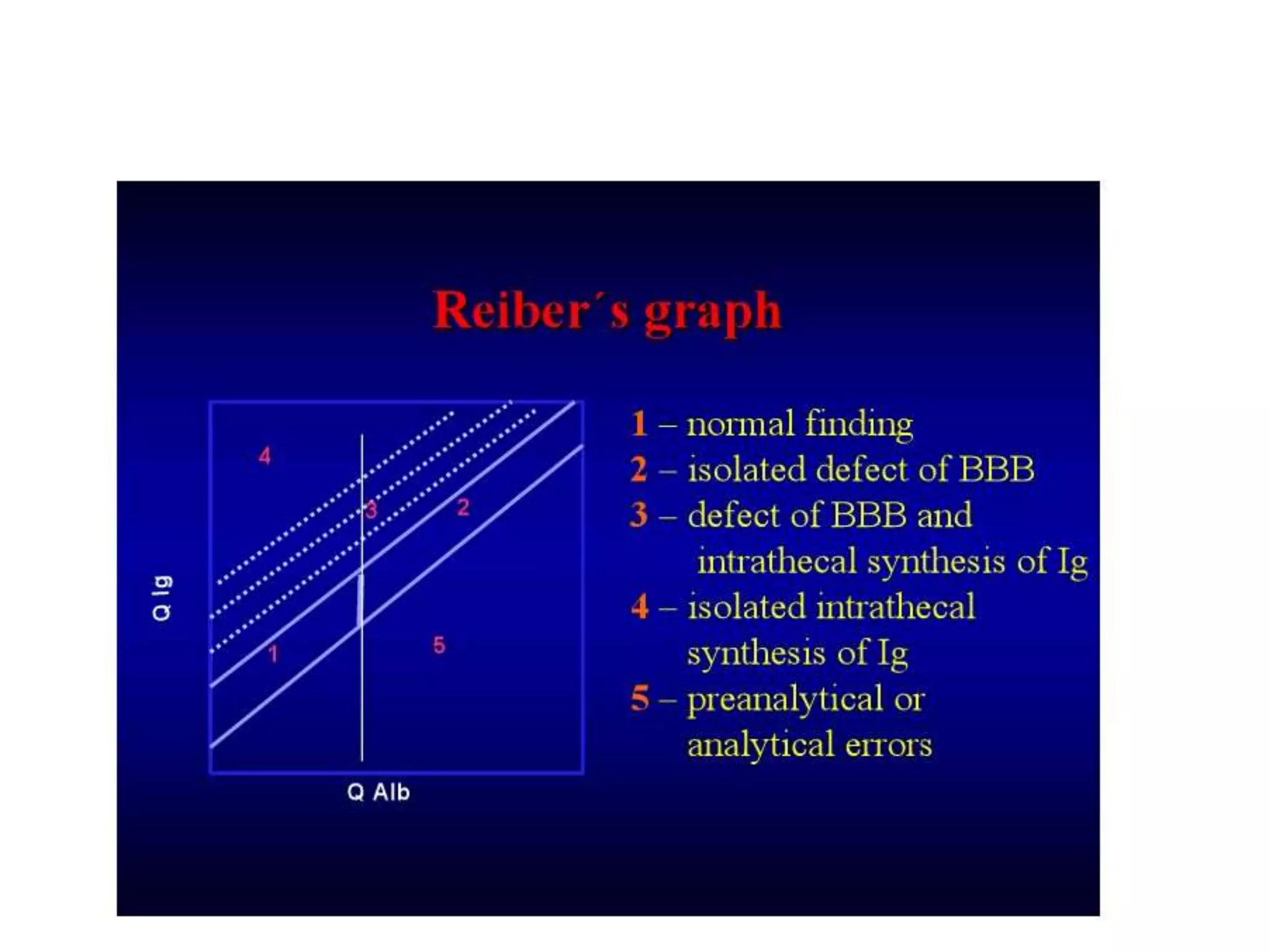
![• FIRST: CHECK INTEGRITY OF BLOOD BRAIN BARRIER (BBB) by
CSF/Serum albumin index calculation:
– CSF serum albumin index = CSF albumin (mg/dl) / serum albumin
(g/dl)
– Index less than 9 indicates intact BBB (no increased permeability of
BBB)
• SECOND: CSF IgG INDEX is calculated:
CSF IgG / Serum IgG
CSF IgG index = ---------------------------------------
CSF albumin / Serum albumin
Normal: less than 0.7
• CSF IgG can arise:
– from plasma cells within CSF and
– from the blood through BBB
• ↑CSF [IgG] without concomitant ↑ in CSF [Alb] suggests local production of IgG:
– multiple sclerosis (MS)
– subacute sclerosing panencephalitis (SSPE)
• Monoclonal IgG in both CSF and Serum – Paraproteins.](https://image.slidesharecdn.com/csfinclinico-laboratorydiagnoses-191004112029/75/Csf-in-clinico-laboratory-diagnoses-21-2048.jpg)



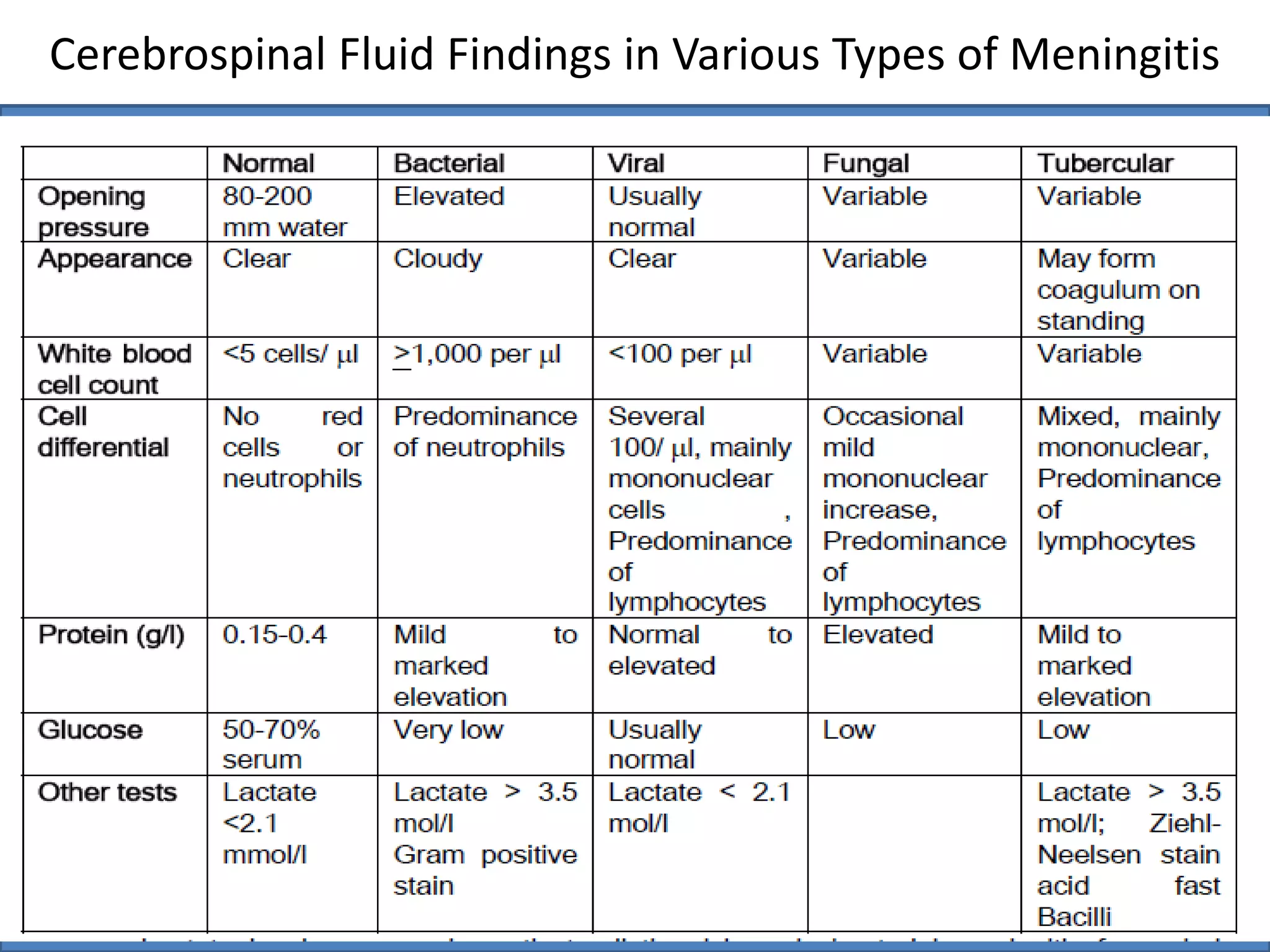
The document summarizes cerebrospinal fluid (CSF) physiology, composition, and analysis. It describes how CSF is produced in the choroid plexus and circulates through the ventricles and subarachnoid space. Normal CSF contains low levels of protein, glucose equal to 60% of plasma, and electrolyte concentrations different than plasma. Analysis of CSF protein, glucose, white blood cells, and other components can help diagnose conditions like meningitis, tumors, and neurological disorders. Increased opening of the blood-brain barrier and local immune responses can be evaluated through analysis of CSF albumin and immunoglobulin levels.















































































