Downloaded 255 times
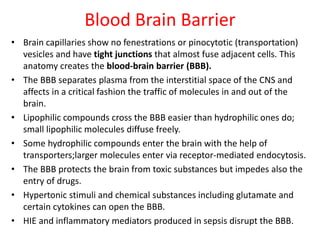
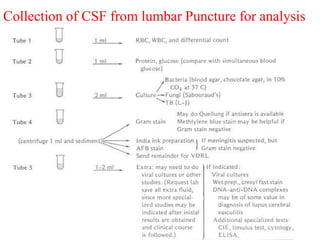
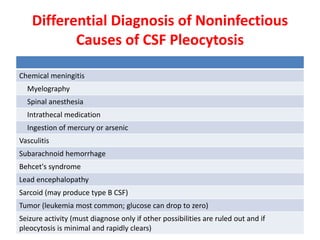
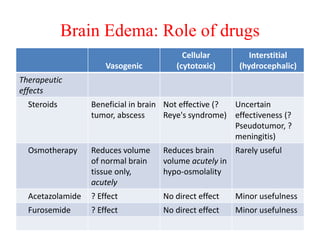
![Proper positioning of a patient in the lateral decubitus position. Note that the shoulders
and hips are in a vertical plane; the torso is perpendicular to the bed. [From RP Simon
et al (eds): Clinical Neurology, 7th ed. New York, McGraw-Hill, 2009.]
Positioning and site of Lumbar puncture](https://image.slidesharecdn.com/csfseminar-140505233255-phpapp02/85/Csf-seminar-27-320.jpg)

![REFERENCES:
• Clinical Methods: The History, Physical, and Laboratory Examinations. 3rd
edition.Walker HK, Hall WD, Hurst JW, editors.Boston: Butterworths; 1990.
• PATHOLOGY 425 CEREBROSPINAL FLUID [CSF] at the Department of Pathology and
Laboratory Medicine at the University of British Columbia. By Dr. G.P. Bondy. Retrieved
November 2011
• Normal Reference Range Table from The University of Texas Southwestern Medical
Center at Dallas. Used in Interactive Case Study Companion to Pathologic basis of
disease.
• Department of Chemical Pathology at the Chinese University of Hong Kong, in turn
citing: Roberts WL et al. Reference Information for the Clinical Laboratory. In Tietz
Textbook of Clinical Chemistry and Molecular Diagnostics, 4th edn. Burtis CA, Ashwood
ER and Bruns DE eds. Elsevier Saunders 2006; 2251 – 2318
• Ballabh P, Braun A, Nedergaard M. The blood-brain barrier: an overview. Structure,
regulation, and clinical implications. Neurobiol Dis 2004;16:1-13. PubMed
• Owens T, Bechman I, Engelhardt B. Neurovascular Spaces and the Two Steps to
Neuroinflammation. J Neuropathol Exp Neurol 2008; 67:1113-21. PubMed
• Aluise CD, Sowell RA, Butterfield DA. Peptides and Proteins in Plasma and Cerebrospinal
Fluid as Biomarkers for the Prediction, Diagnosis, and Monitoring of Therapeutic
Efficacy of Alzheimer’s disease. Biochim Biophys Acta 2008;1782:549-58 PubMed.](https://image.slidesharecdn.com/csfseminar-140505233255-phpapp02/85/Csf-seminar-41-320.jpg)

The document discusses cerebrospinal fluid (CSF), its production, circulation, normal values, functions, and analysis, detailing the clinical significance of CSF characteristics and pathological markers. It covers historical milestones, anatomical aspects, pressure measurements, and various conditions affecting CSF composition and clarity, highlighting the importance of lumbar puncture and its contraindications. Additionally, it outlines CSF biochemical analysis, including proteins, glucose levels, and the implications of findings in different neurological diseases.


![serous fluid Dr shweta [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/serousfluiddrshwetaautosaved-221213040107-a9b2a766-thumbnail.jpg?width=640&height=640&fit=bounds)































![Cytopathology Of Cerebrospinal Fluid[1]Power Point](https://cdn.slidesharecdn.com/ss_thumbnails/cytopathologyofcerebrospinalfluid1power-point-1230479978520994-2-thumbnail.jpg?width=640&height=640&fit=bounds)



















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)








