This document outlines the formation, circulation, and biochemical composition of cerebrospinal fluid (CSF). It discusses how CSF is produced by the choroid plexus in the brain ventricles and absorbed by arachnoid villi. The key functions of CSF include protecting the brain, maintaining homeostasis, and clearing waste. Biochemical analysis of CSF can aid in diagnosing conditions like meningitis, tumors, and subarachnoid hemorrhage. Abnormal levels of glucose, protein, chloride, and cells can provide clues to the pathology. Careful collection and analysis of CSF is important for medical diagnosis and management.
UNIVERSITY OF BUEA
7/22/2019
1
Facultyof Health Sciences
Department of MLS
Chemical Pathology: CPY 602,
BIOCHEMICAL ANALYSISOF CEREBRO-SPINALFLUID
Presented By
Lamngwa Benard Nfor HS18P036
2.
OUTLINE
Introduction
Formation of CSF/anatomy
Circulationof CSF
Functions of CSF
Blood brain barrier
Biochemical composition of CSF
CSF analysis and pathophysiology
Laboratory investigations
Management of some CSF related infections
7/22/2019
2
3.
OBJECTIVES
After this presentation,the students should be able to:
Describe the formation and location of cerebrospinal fluid
(CSF)
Describe the appearance and state the composition of
normal CSF
Understand the formation and functions of CSF
Understand some pathology associated to CSF
Understand biochemical investigations of CSF and
interpretation of such results
Have an idea of management of some related disease
7/22/2019
3
4.
INTRODUCTION
•The cerebrospinal fluid(CSF) is a dynamic,
metabolically active fluid surrounding the brain and
spinal cord and has many important functions.
•It is very valuable as a diagnostic aid in the
evaluation of inflammatory conditions, infections
involving the brain, spinal cord, and
subarachnoid haemorrhage.
7/22/2019
4
5.
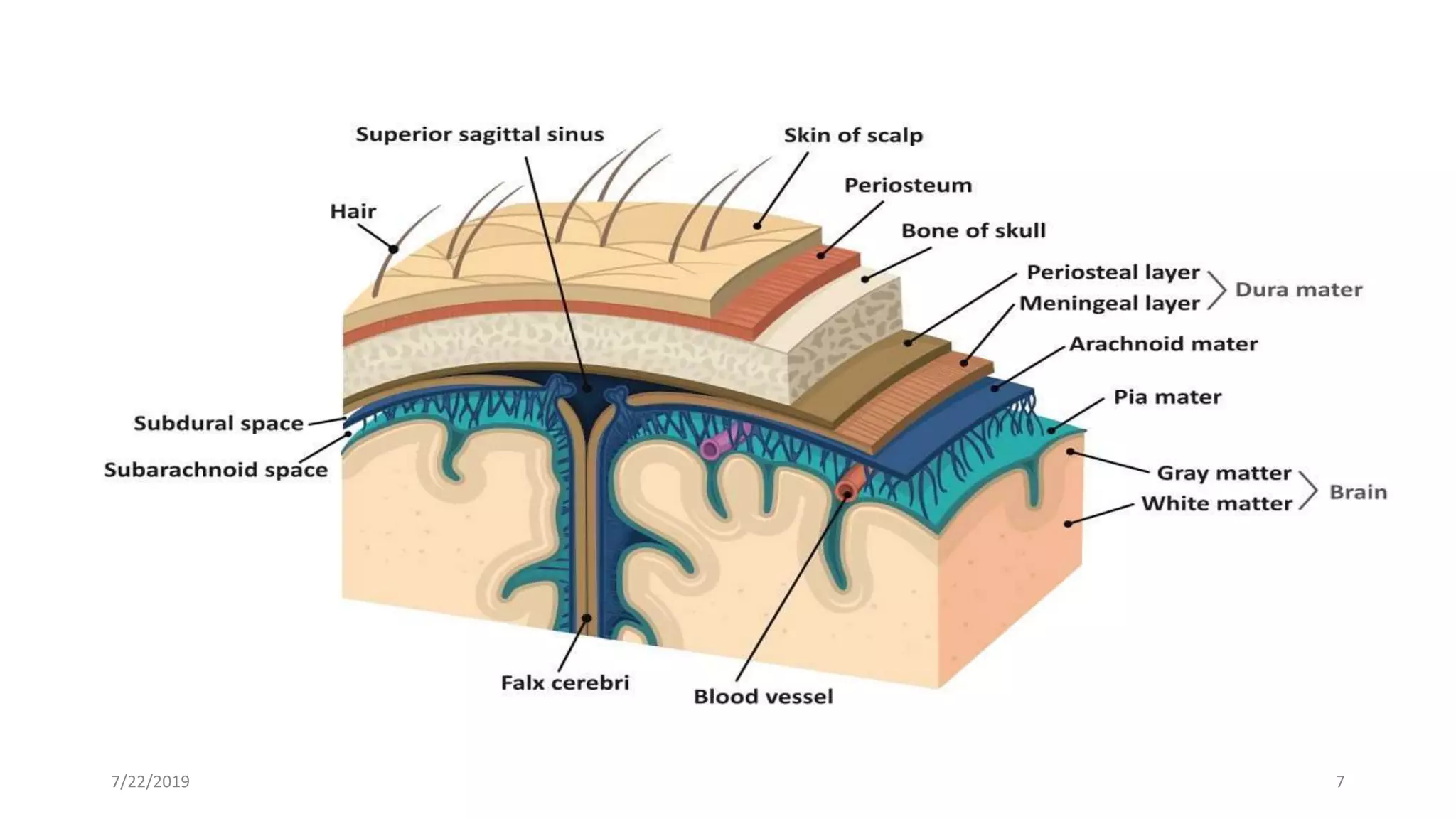
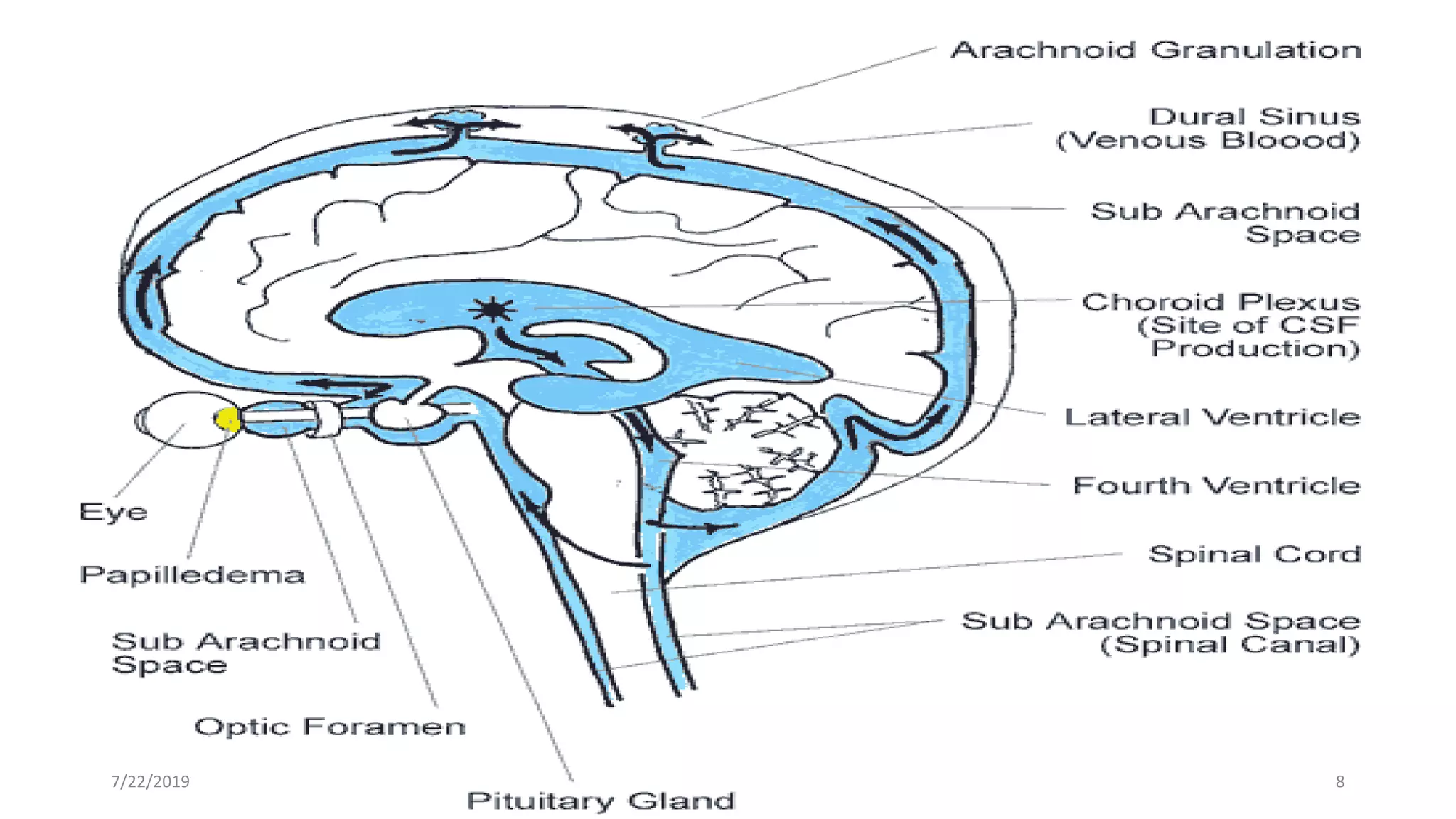
FORMATION OF CSF/ANATOMY
•Boththe brain and spinal cord are covered by three
protective membranes referred to as the meninges. The
outermost layer is called the dura mater and is composed
of tough connective tissue.
•The middle layer is the arachnoid named for it spider web
like appearance.
•The delicate innermost layer which is in direct contact with
the brain and spinal cord is called the pia mater. An
inflammation of the meninges is referred to as meningitis.
7/22/2019 5
6.
FORMATION OF CSFANATOMY CONT.
•Between the arachnoid layer and the pia mater is a space
called the subarachnoid space. It contains a clear, colorless
fluid referred to as Cerebrospinal Fluid (CSF).
•CSF is produced in the ventricles of the brain by a collection
of rich vascular protrusions called the choroid plexus.
•Excess CSF is continuously reabsorbed by arachnoid villi
and returned to the venous system thus maintaining a
consistent amount of fluid under an intracranial pressure
between 50 - 180 mmHg.
7/22/2019 6
FORMATION OF CSF/ANATOMY CONT.
•Generally, the total volume of CSF circulating throughout
the adult Central Nervous System (Brain and Spinal Cord)
is approximately 90 - 150 ml.
•In newborns this volume is 10 -60 ml.
7/22/2019 9
10.
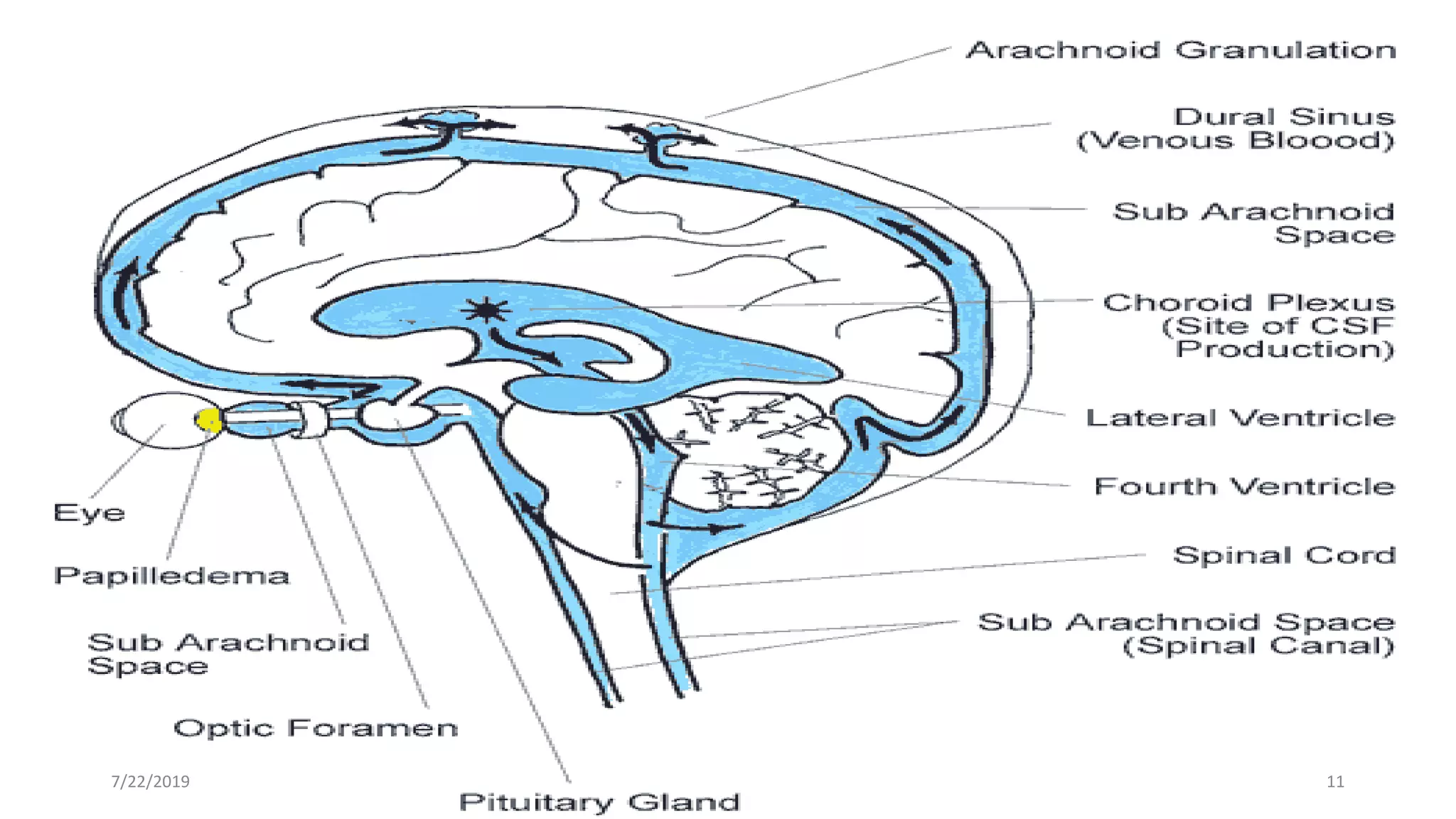
CIRCULATION OF CSF
•CSFflows from the lateral ventricles through the third and
fourth ventricles and into the subarachnoid space.
• From the fourth ventricle, the CSF either continues to the
central canal of the spinal cord or leaves for the
subarachnoid space by passing through the medial aperture
(foramen of Magendie) and paired lateral apertures
(foramina of Luschka) in the roof and lateral recesses of the
fourth ventricle, respectively.
7/22/2019 10
11.
CIRCULATION OF CSF
•CSFflows from the lateral ventricles through the third and
fourth ventricles and into the subarachnoid space.
• From the fourth ventricle, the CSF either continues to the
central canal of the spinal cord or leaves for the
subarachnoid space by passing through the medial aperture
(foramen of Magendie) and paired lateral apertures
(foramina of Luschka) in the roof and lateral recesses of the
fourth ventricle, respectively.
7/22/2019 11
12.
FUNCTIONS OF CSF
•Protection: CSF protects the brain from damage by
buffering the brain. It acts as a cushion
•Buoyancy: The actual mass of the human brain is about
1400 grams;
however, the net weight of the brain suspended in the CSF
is equivalent to a mass of 25 grams. which allows
the brain to maintain its density without being impaired
by its own weight.
7/22/2019 12
13.
FUNCTIONS OF CSFcont.
•Chemical stability/Homeostasis: CSF maintain the
distribution of necessary substance and waste product
between CNS and Blood stream
•Prevention of brain ischemia: made by decreasing the amount
of CSF in the limited space inside the skull. This decreases
total pressure . transport of biomolecules to the brain
•Clearance of catabolites (CO2, lactate)
•Maintenance of constant intracranial pressure
•Clearin of waste: Removes waste from the brain through the
bllod for elimination via kidneys.
7/22/2019 13
14.
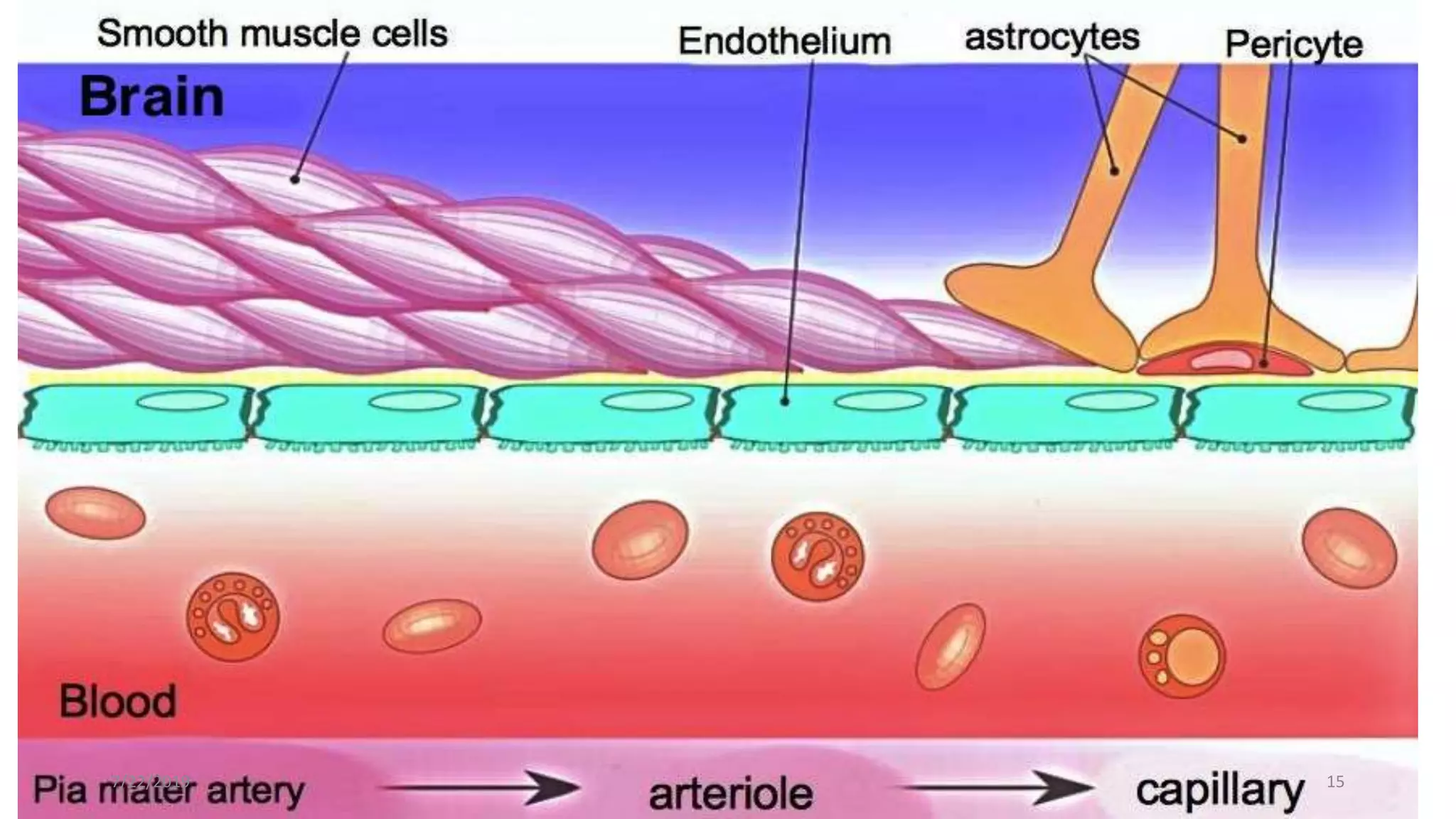
BLOOD BRAIN BARRIER
•.A protective barrier separates the brain from circulating
blood and regulates the distribution of substances between
the blood and the CSF.
• If this protective barrier disrupts, it may result in a change
in the normal level or type of constituents of CSF.
•The blood–brain barrier restricts the passage of pathogens,
the diffusion of solutes in the blood, and large or hydrophilic
molecules into the cerebrospinal fluid (CSF), while allowing
the diffusion of hydrophobic molecules (O2, CO2,
hormones) and small polar molecules.
•Cells of the barrier actively transport metabolic products
such as glucose across the barrier using specific transport
proteins.7/22/2019 14
Collection of CSF
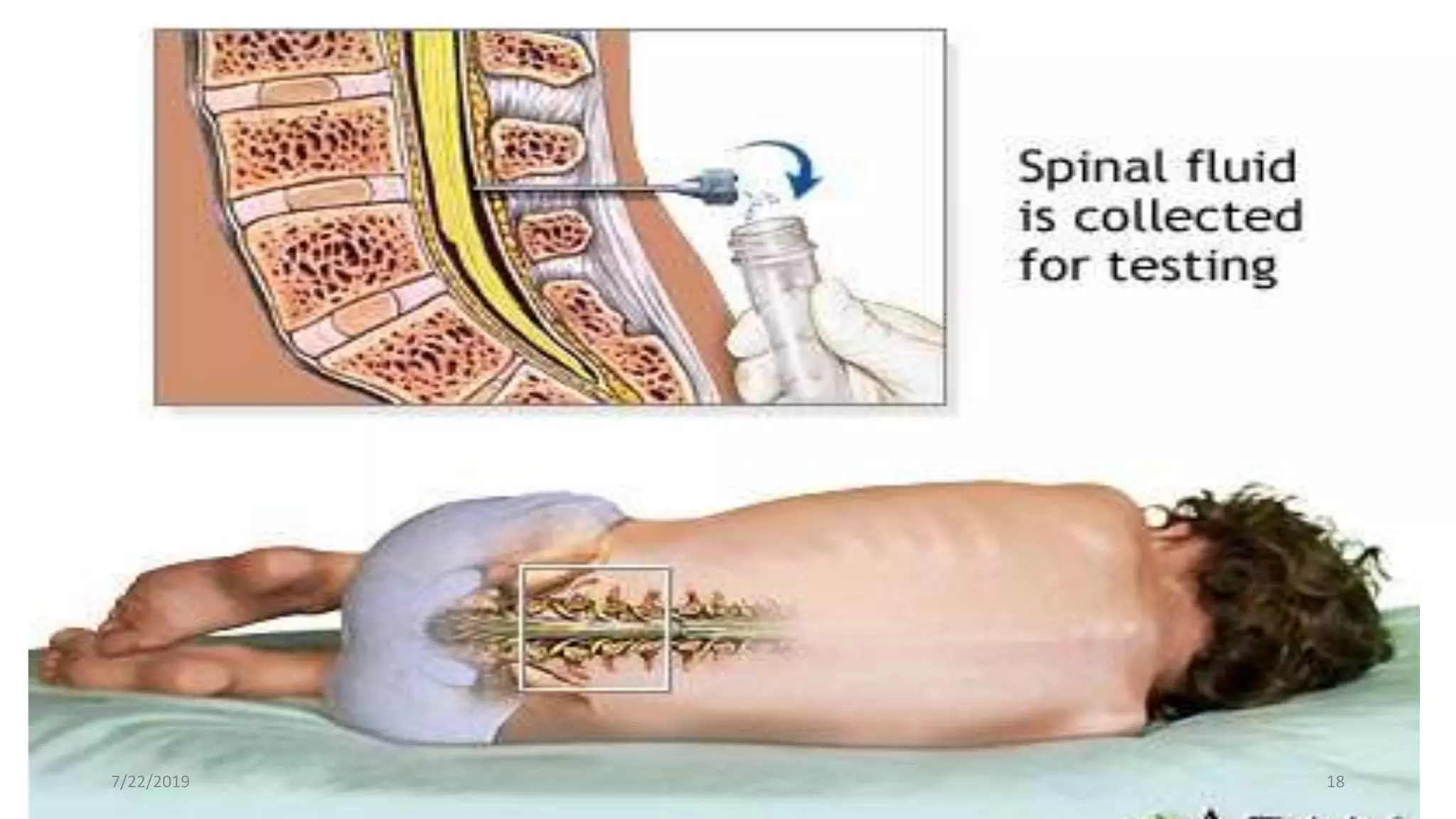
•Thepatient is placed in a lateral position with the knees
bent in full flexion up to the chest(fetal position) (sit and
bend position also possible)
•Introduction of 1% lidocain into the subcutaneous space
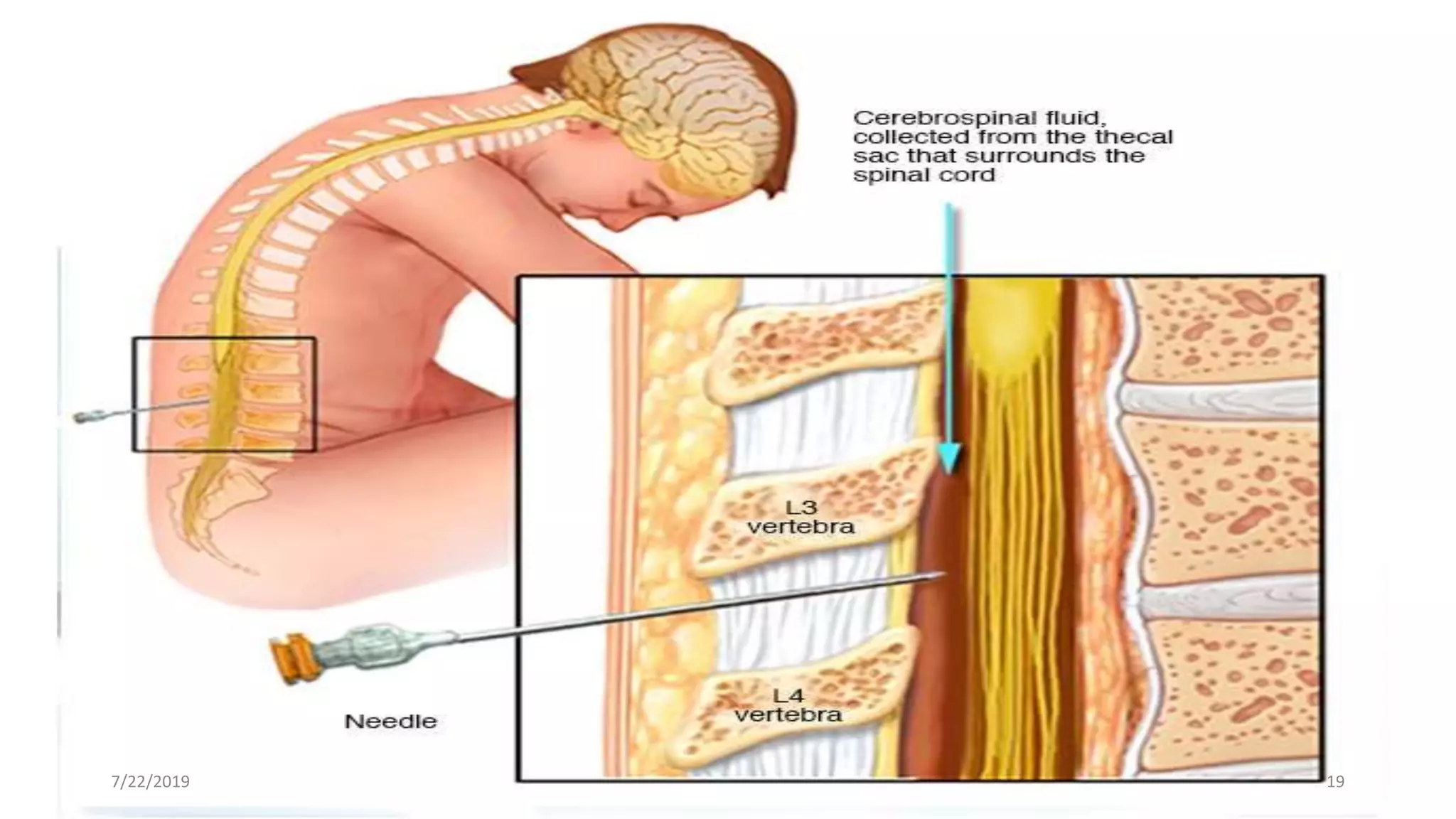
•Insertion of a spinal needle into the subarachnoid space at
the L3-L4 or L4-L5 intercostal spaces (inserted until the
second “give”- subarachnoidal space).
•Removal of the stylet of the needle in order to collect the
fluid
7/22/2019 17
Collection of CSF
•Approximately 10-12 ml can be taken from an adult and
less than 3 ml from a neonate. Care must be taken not to
contaminate the sample with blood.
•The fluid is collected into 3 tubes via free passive flow
through the needle. Up to four tubes of CSF can be
collected aseptically.
•Each tube should contain 2-4 mL of fluid. The tubes should
be labelled with a number indicating the order in which
they were collected. Each tube goes to a different section of
the laboratory for testing
7/22/2019 20
21.
Collection of CSF
•Tube #1 Chemistry: Contains debris from the puncture and
occasionally blood in a "traumatic tap".
Since it is the most likely to be contaminated with microbes, tissue
fluid and blood cells which could yield misleading results. It
is best used for chemistry and immunological
determinations.
• Tube #2 Microbiology. May contain some blood cell contaminants
but is suitable for microbiological studies.
• Tube #3 Haematology. Has the least cellular or debris
contamination and therefore is used for cell counts, white cell
differentials and the examination of abnormal cells e.g. tumor
cells
• Tube #4, Molecular & Reference Lab7/22/2019 21
22.
CSF ANALYSIS ANDPATHOPHYSIOLOLOGY
• CSF is investigated to aid in the diagnosis of SAH
(subarachnoid hemorrhage), Meningitis, Demyelinating
disorders, CNS malignancy, Head injury with CSF leak and
other less common tests, the majority of the investigations
involve cytology and microbiology and chemistry.
•Meningitis
•Can be bacterial ( pyogenic or tuberculous), viral or fungal
( Cryptococcus). Apart from direct organism identification,
biochemistry and cell counts can help distinguish between
the types of meningitis.
7/22/2019 22
23.
CSF ANALYSIS ANDPATHOPHYSIOLOGY cont.
• In classical pyogenic meningitis ( eg Strep
Cryptococcal) CSF protein levels are high > 0.8 g/L,
glucose is much lower than 60% of blood value, high
counts of PMNL’ s ( polymorphonuclear lymphocytes)
occur and the CSF is turbid.
•TBM (tuberculous meningitis) can be differentiated by a
mixed PMNL/lymphocyte high cell count and a low CSF
chloride.
•Viral meningitis often has a lymphocytosis with a normal
glucose, normal protein levels and a clear CSF.
•Fungal infections present with CSF lymphocytosis, a high
protein count and normal glucose
7/22/2019 23
CSF ANALYSIS ANDPATHOPHYSIOLOGY cont.
• CSF GLUCOSE
•Glucose enters the CSF from the plasma by 2 mechanisms,
diffusion and active transport. Glucose is the primary
source of energy for the brain. Brain is 5 % body mass but
uses 20% glucose.
•The level of CSF glucose is influenced by the concentration
and duration of the plasma glucose level.
•CSF glucose levels are roughly two-thirds of plasma
glucose levels
•CSF glucose can only be interpreted reliably with a blood
sample taken within 15 min before or after an LP.
7/22/2019 25
26.
CSF ANALYSIS ANDPATHOPHSIOLOGY cont.
CSF CHLORIDE
The diagnosis of tuberculous meningitis is notoriously
difficult to make. Chloride (less than 110mmol/1) is used to
distinguish tuberculous from viral and bacterial meningitis.
A CSF chloride of less than 100mmol/l is thought to be
virtually diagnostic of TBM.
CSF PROTEIN. Spinal fluid is an ultrafiltrate of plasma
that lacks high molecular weight proteins such as beta
lipoprotein, alpha-2 macroglobulin, IgM, etc.
7/22/2019 26
27.
CSF ANALYSIS ANDPATHOPHYSIOLOGY cont.
Measurement of CSF protein is also used to
distinguish septic from aseptic meningitis.
Protein concentrations >1 g/L are often viewed as
diagnostic for bacterial, fungal, or tuberculous meningitis,
reflecting the presence of the pathologic organism
Unfortunately, the increase of CSF protein is a sequela in
many CNS disease processes, usually in association with
increased permeability of the bloodbrain barrier, vasogenic
brain edema, hypercellularity, and release of brain-specific
proteins during cell death
7/22/2019 27
28.
CSF ANALYSIS ANDPATHOPHYSIOLOGY cont.
SUBARACHNOID HAEMORRHAGE
In subarachnoid haemorrhage red cells are a diagnostic
feature in the CSF, so careful LP is essential.
Red cells that have been in the CSF for longer than 4
hours cause a yellow staining of the CSF called
xanthochromia and the presence of this in fresh CSF
confirms bleeding into the subarachnoid space from a
source other than contamination during the LP. Keep in
mind that there are other causes of
xanthochromia. Xanthochromia refers to a yellow, orange
or pink colour7/22/2019 28
29.
CSF ANALYSIS ANDPATHOPHYSIOLOGY
cont.
HEAD INJURY
• In patients with rhinorrhoea or otorrhoea, post head
injury or spontaneously, it is important to ascertain
whether CSF is present in the fluid, which would
confirm a CSF leak. This is done by identifying beta-
2-transferrin in the fluid leak sample, using
electrophoresis and immunofixation
7/22/2019 29
30.
CSF ANALYSIS ANDPATHOLOGY cont.
• Protein index:
• This assesses the amount of intrathecal protein synthesis that may
occur in an inflammatory disease and assesses the permeability of
the blood-brain barrier in relation to increased intrathecal synthesis
(eg IgG).
• Albumin is used as a reference protein.
• A normal CSF Albumin/Serum Albumin ratio is less than 9. CSF
IgG index = CSF IgG/Serum IgG ÷ CSF Albumin/Serum Albumin
Usually the CSF IgG index will be 0.3-0.8. If > 0.8, this indicates
increased intrathecal synthesis such as may be seen in multiple
sclerosis..
7/22/2019 30
31.
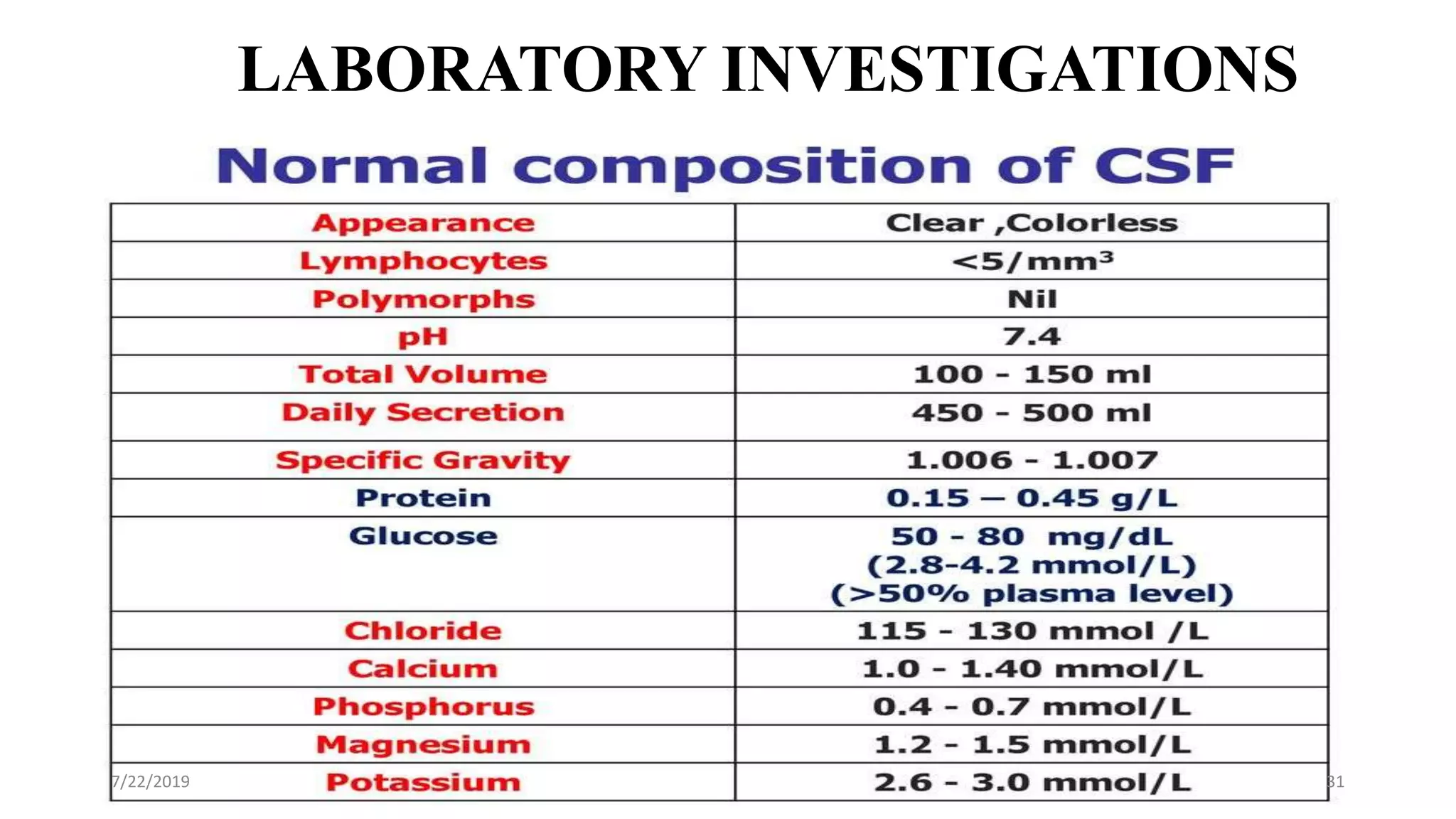
LABORATORY INVESTIGATIONS
• Physicalexamination
•Normal CSF is:
•Colorless
•Clear
•Free of clots
•Free of blood
•If CSF is cloudy (turbid) ,
perform microscopic
examination:
•Usually due to leucocytes
•may be due to micro-
organisms
7/22/2019 31
32.
LABORATORY INVESTIGATIONS
• Physicalexamination
•Normal CSF is:
•Colorless
•Clear
•Free of clots
•Free of blood
•If CSF is cloudy (turbid) ,
perform microscopic
examination:
•Usually due to leucocytes
•may be due to micro-
organisms
7/22/2019 32
33.
Blood & Hemoglobinpigments in CSF
Traumatic tap
•bright red color
• RBCS in decreasing
number as the fluid is
sampled
Subarachnoid hemorrhage
(SAH)
•Xanthochromia
(hemoglobin breakdown
pigments) = RBCs lysis &
metabolism previously
occurred (at least 2 hr
earlier)
7/22/2019 33
34.
Examination of CSF
(Biochemicalanalysis of CSF)
•Tests of interest:
•Glucose
•Protein
Total
Specific:
Albumin
Immunoglobulin
Others (e.g. myelin basic protein; MBP)
Lactate
7/22/2019 34
35.
Glucose
• Glucose entersCSF via facilitative transporter (GLUT)
• CSF glucose is ~ 2/3 that of plasma 50 - 80 mg/dl
• A plasma sample must be obtained ~ 2-4 hr before CSF
sample
• In hypoglycemia, CSF glucose may be very low and In
hyperglycemia glucose is raised.
• Measure CSF Glucose immediately or preserve the
specimen with and antiglycolytic
7/22/2019 35
36.
Glucose
•↑ CSF glucoseconc. (hyperglycorrhachia) :
•Not clinically informative
•Provides only confirmation of hyperglycemia
•↓CSF [glucose] (hypoglycorrhachia):
1)Disorder in carrier-mediated transport e.g. TB meningitis,
2)Active metabolism of glucose by cells or organisms:
•e.g. acute purulent, amebic, & fungal meningitis
3)Increased metabolism by the CNS
4)Glucose is measured by the use of a Spectrophotometer
7/22/2019 36
37.
Proteins
•The Proteins mostlyfound in the CSF is albumin
•Source of CSF proteins:
• 80% from plasma by ultrafiltration
• 20% from intrathecal synthesis
7/22/2019 37
38.
proteins cont.
•Increase CSFtotal protein
Must be compared to the serum protein conc.
Useful nonspecific indicator of pathological states:
•Lysis of contaminant blood (traumatic tap)
•↑ Permeability of the epithelial membrane due to:
•Bacterial or fungal infection, cerebral hemorrhage
•↑ production by CNS tissue in, e.g Multiple sclerosis
(MS)
•Obstruction e.g. in tumors and abscess
7/22/2019 38
39.
Proteins cont.
•Total proteinis measured spectrophotometrically
•The Pandys test is also used for the qualitative
detection of total protein in CSF
7/22/2019 39
40.
Albumin
• Albumin isproduced solely in the liver
• Its presence in CSF must occur through BBB
• Measured by the protein electrophoresis method
7/22/2019 40
41.
Immunoglobulin
• CSF IgGcan arise:
• from plasma cells within CSF
• from the blood through BBB
•Increase IgG conc. and normal Alb conc. of CSF
suggests local production of IgG, e.g.,
• Multiple sclerosis (MS)
• Subacute sclerosing panencephalitis (SSPE)
• IgG can be measured by electrophoretic method
• Also measured by immunoassays.
7/22/2019 41
42.
Management of CSFrelated infections
Meningitis
Bacterial meningitis is a medical emergency
Empirical selection of therapy is usually necessary, and
treatment should be started at the first suspicion of bacterial
meningitis.
A single dose of benzylpenicillin can be given if the person is
outside hospital, but cefotaxime is the preferred treatment in
hospital
Chloramphenicol is an option for those who have an allergy to
both penicillin and cephalosporins.
Treatment is given for 5 days for meningococcus, and 10 days
for Haemophilus influenzae or pneumococcus.
7/22/2019 42
43.
Management of CSFrelated infections
Meningitis
Amphotericin is active against all common fungi that cause
systemic infection (Candida, Aspergillus, Mucor and
Cryptococcus species). Cryptococcus is incriminated in
cryptococcal meningitis.
Tuberculosis is usually treated with a multidrug regimen because
of the rapid development of resistance. Rifamycins (rifabutin,
rifampicin), Isoniazid, Pyrazinamide and Ethambutol are first line
regimen.
Other drugs can be used as second-line treatments in multidrug-
resistant tuberculosis. These include cycloserine, capreomycin,
amikacin, ciprofloxacin, moxifloxacin, azithromycin,
clarithromycin and p-aminosalicylic acid7/22/2019 43
44.
Management of CSFrelated infections
Acute brain injury
Mannitol is occasionally used to reduce ischaemic cerebral
damage, for example after neurosurgery or in acute traumatic
brain injury.
Fluid loss via the kidney should be replaced with
intravenous crystalloid to avoid dehydration.
Dexamethasone is often used to reduce oedema
around malignant tumours in the brain and those
compressing the spinal cord
7/22/2019 44

![Glucose
•↑ CSF glucose conc. (hyperglycorrhachia) :
•Not clinically informative
•Provides only confirmation of hyperglycemia
•↓CSF [glucose] (hypoglycorrhachia):
1)Disorder in carrier-mediated transport e.g. TB meningitis,
2)Active metabolism of glucose by cells or organisms:
•e.g. acute purulent, amebic, & fungal meningitis
3)Increased metabolism by the CNS
4)Glucose is measured by the use of a Spectrophotometer
7/22/2019 36](https://image.slidesharecdn.com/laboratoryanalysisofcsf-190722131552/75/Laboratory-analysis-of-csf-36-2048.jpg)