
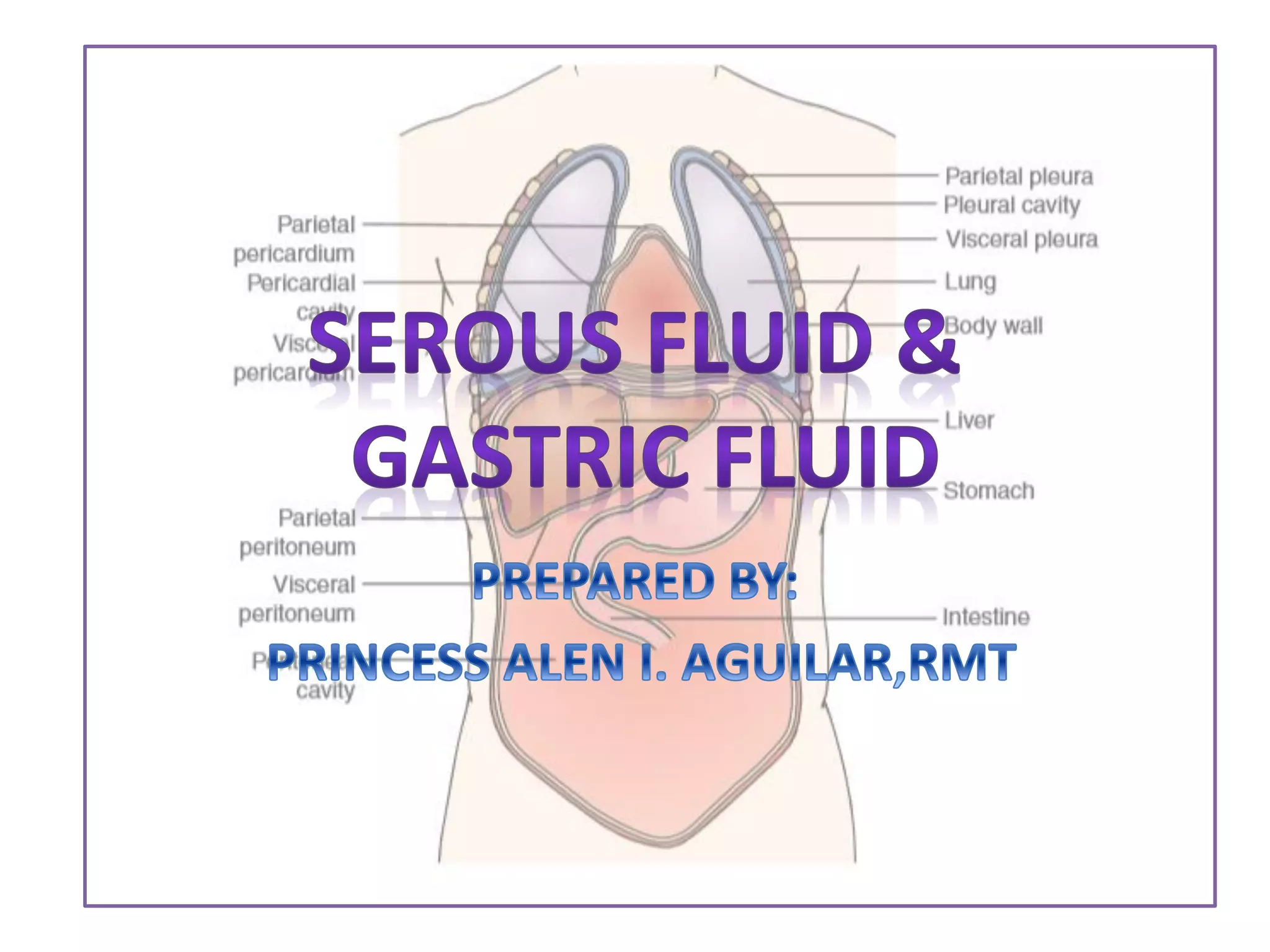
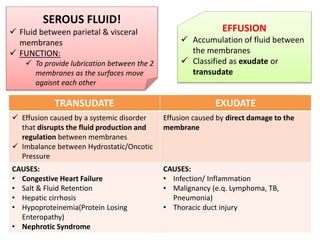
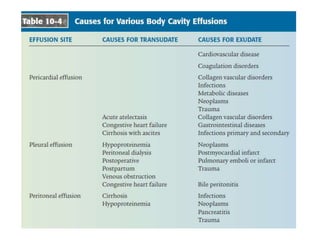
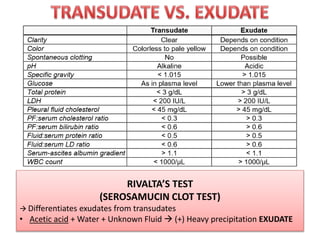
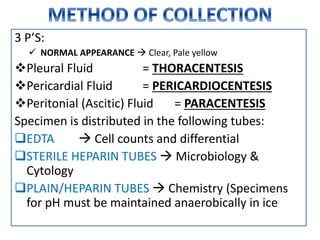
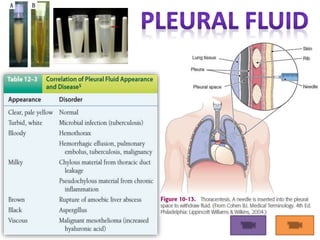

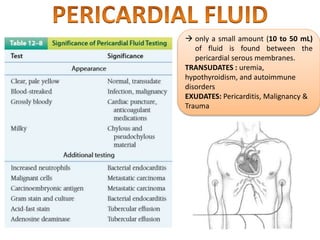
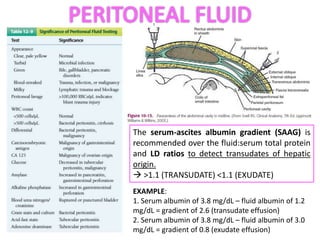



This document provides information on serous fluid, effusions, and tests used to analyze body fluids. It discusses: - Serous fluid's function of lubricating membranes and effusions occurring when fluid accumulates between membranes. Effusions are classified as transudates or exudates. - Causes of transudates include systemic disorders, while exudates are caused by direct membrane damage from infection, inflammation, or malignancy. - The Rivalta's test differentiates exudates from transudates based on precipitation with acetic acid and water.



![serous fluid Dr shweta [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/serousfluiddrshwetaautosaved-221213040107-a9b2a766-thumbnail.jpg?width=640&height=640&fit=bounds)













































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)





