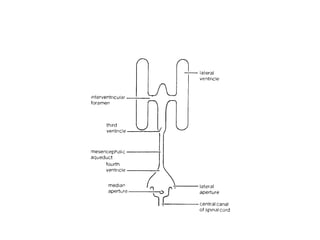
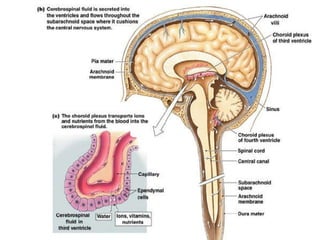
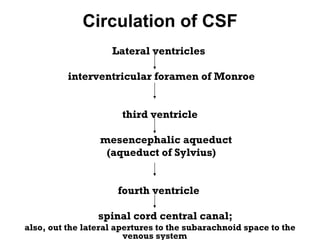
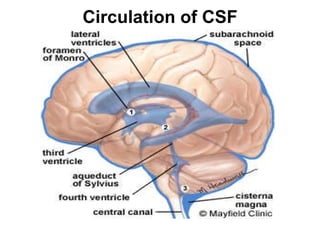
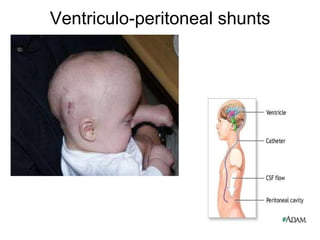
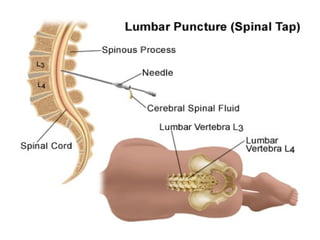
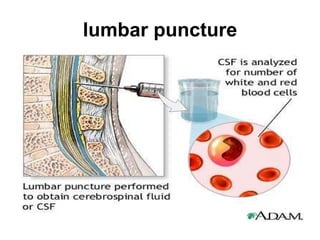
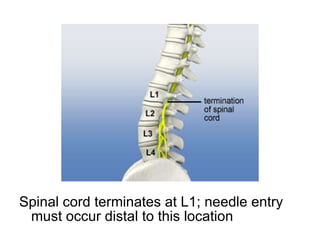
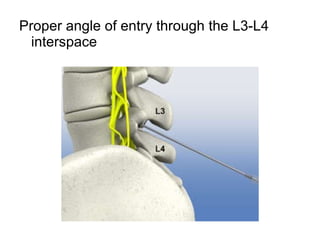
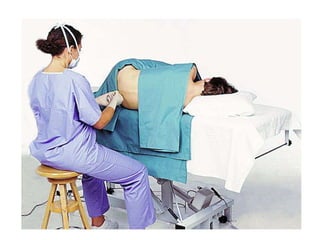
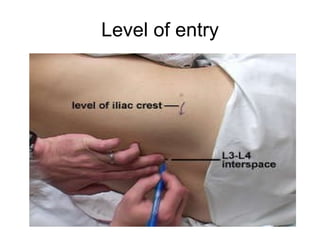
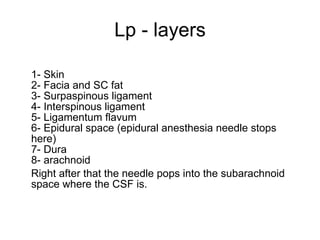
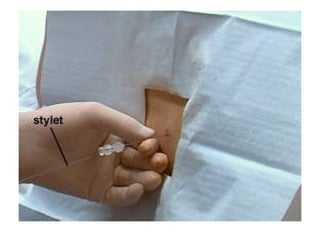
The document discusses cerebrospinal fluid (CSF), including its location in the brain and spinal cord, how it is produced and circulated, its composition and functions. CSF acts as a cushion and protects the brain, removes waste, and transports nutrients and chemicals. It is produced in the brain's ventricles and circulates through the ventricles and spinal cord before being reabsorbed or drained into veins. Abnormalities in CSF production or circulation can cause hydrocephalus. A lumbar puncture is described as a way to collect and analyze CSF samples for diagnostic purposes.


































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)








