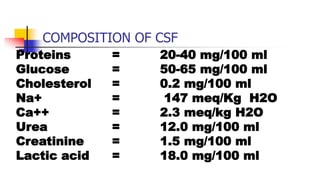
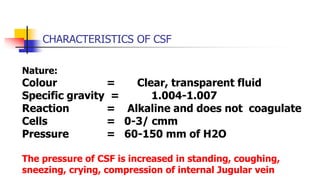
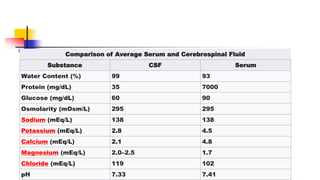
Cerebrospinal fluid (CSF) is a clear fluid that surrounds the brain and spinal cord. It is produced by specialized cells in the brain and acts as a cushion and filtration system. CSF composition is tightly regulated by the blood-brain barrier to protect the central nervous system. CSF analysis through lumbar puncture is important for diagnosing conditions like meningitis, tumors, and multiple sclerosis. Abnormalities in CSF properties including white blood cell count, glucose, protein, and presence of tumor cells or blood can indicate different diseases.

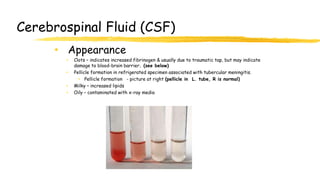
![CEREBROSPINAL FLUID[CSF]
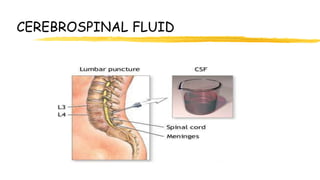
The cerebrospinal Fluid is a clear, colorless
transparent, tissue fluid present in the
cerebral ventricles, spinal canal, and
subarachnoid spaces.](https://image.slidesharecdn.com/cerebralspinalfluid-220731024045-e07b0b3f/85/Cerebral-Spinal-Fluid-pptx-5-320.jpg)
![CEREBROSPINAL FLUID [FORMATION]
CSF is largely formed by the choroid plexus of the lateral
ventricle and remainder in the third and fourth ventricles.
About 30% of the CSF is also formed from the ependymal
cells lining the ventricles and other brain capillaries.
The choroid plexus of the ventricles actively secrete
cerebrospinal fluid.
The choroid plexuses are highly vascular tufts covered by
ependyma.](https://image.slidesharecdn.com/cerebralspinalfluid-220731024045-e07b0b3f/85/Cerebral-Spinal-Fluid-pptx-8-320.jpg)
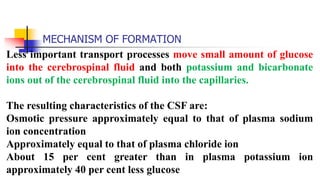
![MECHANISM OF FORMATION OF CSF
Rate of formation:
About 20-25 ml/hour
550 ml/day in adults. Turns over 3.7 times a day
Total quantity: 150 ml:
30-40 ml within the ventricles
About 110-120 ml in the subarachnoid space [of which
75-80 ml in spinal part and 25-30 ml in the cranial part].](https://image.slidesharecdn.com/cerebralspinalfluid-220731024045-e07b0b3f/85/Cerebral-Spinal-Fluid-pptx-12-320.jpg)
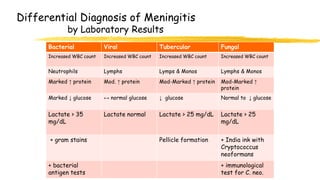
![CSF AND INFLAMMATION
Increased inflammatory cells [pleocytosis] may be caused
by infectious and noninfectious processes.
Polymorphonuclear pleocytosis indicates acute suppurative
meningitis.
Mononuclear cells are seen in viral infections
(meningoencephalitis, aseptic meningitis), syphilis,
neuroborreliosis, tuberculous meningitis, multiple sclerosis,
brain abscess and brain tumors.](https://image.slidesharecdn.com/cerebralspinalfluid-220731024045-e07b0b3f/85/Cerebral-Spinal-Fluid-pptx-24-320.jpg)
![CSF AND PROTEINS
Multiple sclerosis: CSF protein is normal or mildly
increased.
Increased IgG in CSF, but not in serum [IgG/albumin index
normally 10:1].
90% of MS patients have oligoclonal IgG bands in the CSF.
Oligoclonal bands occur in the CSF only not in the serum.
The CSF in MS often contains myelin fragments and myelin
basic protein (MBP).
MBP can be detected by radioimmunoassay. MBP is not specific for
MS. It can appear in any condition causing brain necrosis, including
infarcts.](https://image.slidesharecdn.com/cerebralspinalfluid-220731024045-e07b0b3f/85/Cerebral-Spinal-Fluid-pptx-27-320.jpg)
![CSF AND XZNTHOCHROMIA
Xanthochromia [blonde color] of the CSF
following subarachnoid hemorrhage is due to
oxyhemoglobin which appears in 4 to 6 hours and
bilirubin which appears in two days.
Xanthochromia may also be seen with hemorrhagic
infarcts, brain tumors, and jaundice.](https://image.slidesharecdn.com/cerebralspinalfluid-220731024045-e07b0b3f/85/Cerebral-Spinal-Fluid-pptx-30-320.jpg)














































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)







